
When I was a med student, I couldn't wrap my head around AKI. Yet, it seemed like every patient had one! Learn these key pearls and follow the @pointofcaremed inpatient AKI template to help master the topic! - Thread - #MedEd #MedTwitter #FOAMed #tipsfornewdocs 1/28
You can find the template and pearls here: https://www.pointofcaremedicin... Also check out the accompanying podcast and YouTube channel, which includes slides. https://anchor.fm/pointofcarep... https://youtu.be/tssoeaZzX54 2/28
First, some definitions of AKI: - rise in serum Cr >0.3 over 48 hours - rise in serum Cr >1.5x baseline over 1 week - UOP < 0.5 cc/kg/hr over 6 hours Frankly, these definitions didn't do much to help me understand AKI. 3/28
It didn't click until someone showed me the picture below. There is a non-linear relationship between creatinine and GFR. At lower creatinine levels, a small increase represents a significant decrease in GFR. 4/28
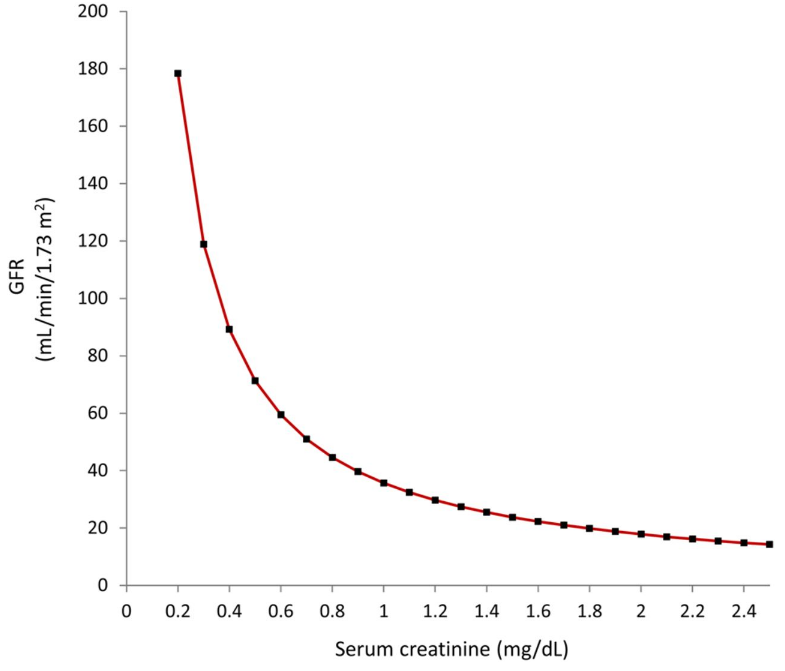
In other words, going from creatinine 0.5 to 1.0 is way more clinically significant than going from 1.5 to 2.0. In both scenarios, creatinine increases by 0.5 (and thus both are technically AKI), but the first indicates a 100% change from baseline and ~50% decrease in GFR. 5/28
Creatinine is a product of muscle breakdown, and levels vary based on diet and muscle mass. Cystatin C is made by all cells with nuclei, and it can be a better way to measure GFR. Note that GFR is validated in CKD, not AKI. https://pubmed.ncbi.nlm.nih.go... 6/28
Here's my checklist for admitting a patient with AKI. It includes what to look for on a chart check, things to ask during an HPI intake, some "can't miss" diagnoses, orders to place, and what initial treatment you should consider. 7/28
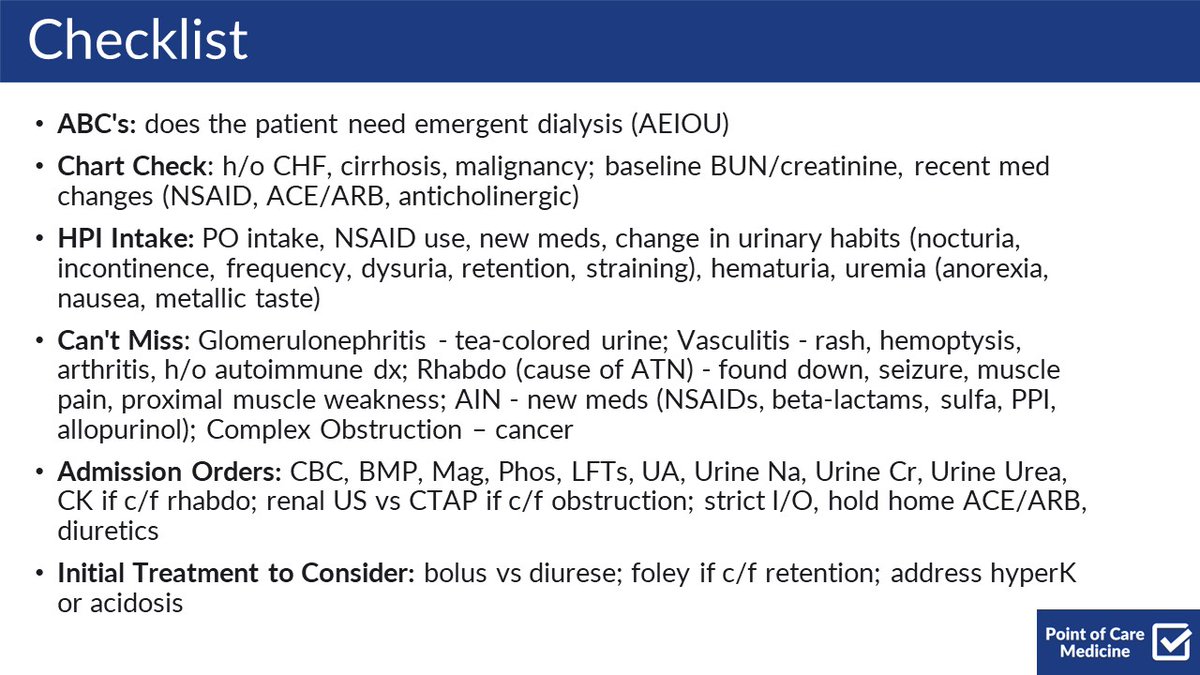
Some highlights of the checklist: - know emergent dialysis indications (more on this later) - know if pt has a reason to be overloaded - new meds - esp NSAIDs and ACE/ARB - changes in urinary habits esp retention - consider "can't miss" diagnoses (send UA) 8/28
As a student, I tried to remember all the zebras for my ddx but they are so difficult to keep straight. In practice, the vast majority of presentations are due to a prerenal etiology or ATN. Here's my framework for common inpatient causes of AKI. 9/28

Prerenal AKI is caused by decreased renal perfusion and thus decreased GFR whereas intrinsic AKI is due to direct damage to the kidney. One point of confusion is that prolonged or profound prerenal physiology can lead to intrinsic injury via ischemia and tubular necrosis. 10/28
Based on common things being common, most inpatient AKIs are fixed by fluid, lasix, or a foley. Fluid - hypotension, pre-renal Lasix - CHF, pre-renal Foley - retention or BPH, post-renal On the other hand, if it's ATN, the only therapy is patience. 11/28
Unless the patient is overloaded or has known h/o CHF, ESRD, cirrhosis, etc it's usually okay to trial 500-1000cc of fluid. If the AKI resolves within 48 hours, it was probably hypovolemia, and you're done. 12/28
That being said, as a general rule of thumb, it's easier to get fluid into a patient than out of them, so if there is any evidence that the patient is not making urine or may become overloaded with pulm edema, you should be more cautious with fluid. 13/28
Here's a sample workup. Everyone gets UA. Urine studies are easy enough to send, though admittedly not always useful. Imaging if c/f obstruction to check for anatomy and hyronephrosis. Sometimes glomerular workup or biopsy if high concern or rapidly progressive disease 14/28
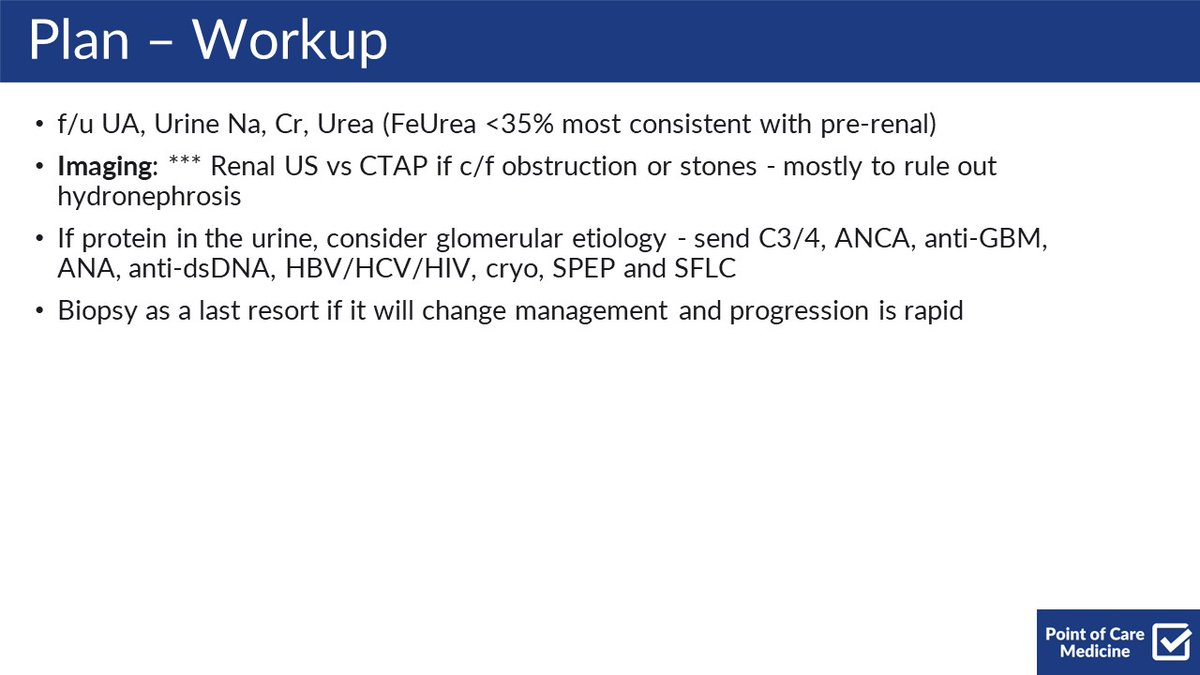
As a student, I took the BUN/Cr ratio as gospel. Classically, >20 is prerenal and < 20 is intrarenal. But why? Note that the following descriptions are simplified so I can keep them straight in my mind, but the physiology is far more complex. 15/28
When healthy, the kidney re-absorbs more BUN than creatinine. In intrarenal AKI, this ability to re-absorb is lost, BUN levels in the blood go down, thus lowering the ratio to <15-20. Note, however, that a "normal" ratio can be anwywhere from 5-20 16/28
In prerenal AKI, the kidney believes the body is volume-down (whether it is or not) and so activates RAAS. RAAS leads to the absorption of Na, H2O, AND BUN. Thus, the BUN/Cr ratio increases. This is also why the fractional excretion of Na is <1% and of Urea is <35%. 17/28
HOWEVER, such urine studies are often useless and must be interpreted with caution. These general cutoffs assume that the patient has not received fluid or diuretics. And how often does that happen in practice? As always, they should be just one part of your assessment. 18/28
That being said, a urinalysis is a great way to get a gut check for some "can't miss" diagnoses. Some examples: Blood with RBCs - nephritis, stone Blood without RBCs - myoglobin/rhabdo Protein - glomerular etiology, vasculitis, SLE WBCs - AIN, infection 19/28
Here is a sample template for treatment options. One major decision point is fluids vs diuresis - trust your exam and clinical judgment. Unless driven by overload and CHF, diuretics and ACE/ARBs should usually be held. NSAIDs should generally be avoided in all cases. 20/28
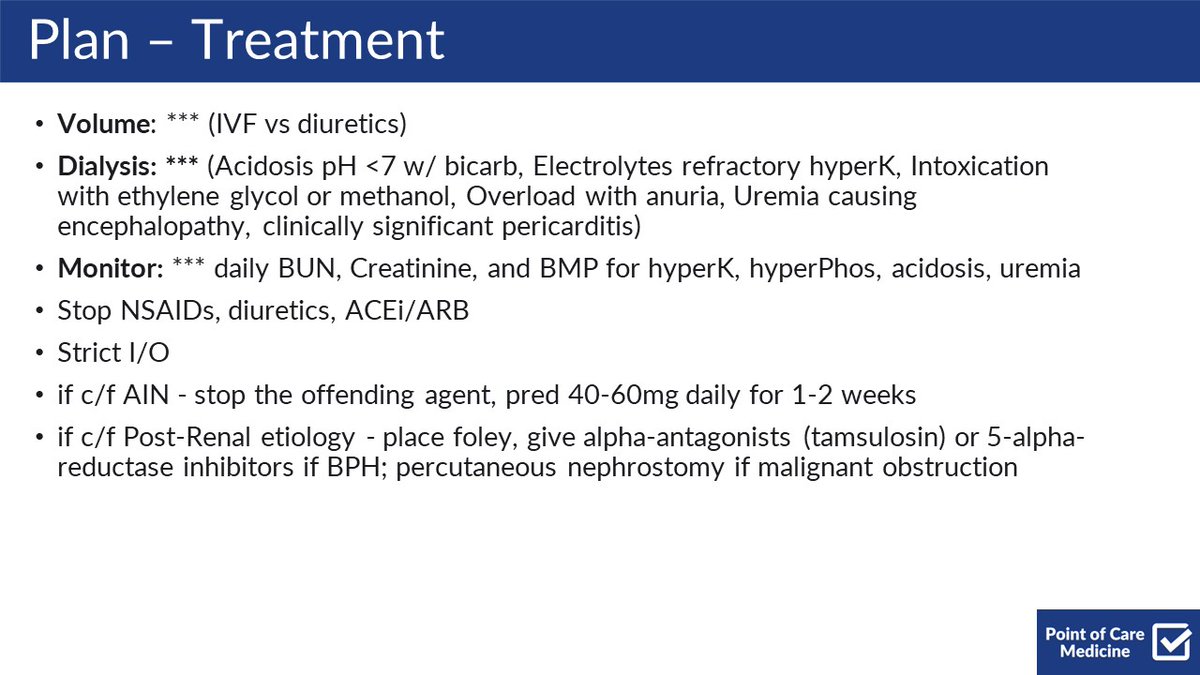
The emergent indications for dialysis: Acidosis - pH <7 despite temporizing measures Electolytes - refractory hyperK Intoxication - ex: ethylene glycol, methanol Overload - w/ anuria and c/f pulm edema Uremia - if causes clin sig encephalopathy or pericarditis 21/28
As a student, I took the AEIOU indications as hard and fast rules. In reality, patients rarely get "emergent" dialysis unless they are already on dialysis and have missed sessions. To me, this is its own unique presentation. See this template: https://www.pointofcaremedicin... 22/28
Why do ACE/ARBs and NSAIDs cause AKI? ACE/ARBs - decrease RAAS - less Na and H2O absorbed, leading to prerenal physiology and lower BP NSAIDs - afferent arteriole constriction decreases flow and thus GFR causing pre-renal physiology. They can also cause AIN! 23/28
One of the hardest parts of managing AKI is being able to spot ATN and being comfortable with waiting for the kidney to heal. I also never understood what was going on with ATN auto-diuresis/polyuria. It only makes sense to me if I again simplify the complex physiology. 24/28
In ATN, there is an acute decrease in GFR leading to lower UOP. Glomerular filtration recovers faster than tubular reabsorption. In other words, the GFR returns, but the filtrate flows right past the healing tubules. This leads to the polyuria. It can last for weeks. 25/28
Lastly, venous injections of contrast are very unlikely to cause intrarenal AKI. You should get the scan if it's clinically indicated. @PulmCrit and @emcrit have done a deep dive on the topic that everyone should read https://emcrit.org/ibcc/contra... 26/28
Other amazing resources: @CPSolvers AKI schemas The excellent review of creatinine, cystatin C, and GFR co-authored by none other than The Sheriff of Sodium! @jbcarmody https://pubmed.ncbi.nlm.nih.go... 27/28
If you remember nothing else... Play the odds - think prerenal or ATN Treatment is most commonly fluids, lasix, or a foley Only treatment for ATN is patience Take urine studies with a grain of salt UA can help with some "can't-miss" diagnoses AEIOU 28/28
AKI is an amazingly complex topic and this was just a snapshot of some high-yield concepts for inpatient management. @Mark_Heslin @bharatbalan @lukasronnerMD @ASanchez_PS What would you guys add? Any pearls, literature, or other resources you like?
You can check out the @GlassHealthHQ page I made highlighting this material for the workup and management of inpatient AKI. https://glass.health/pages/851...
I hope you've found this thread valuable! Follow me @ROKeefeMD for more clinical threads and pearls. Like/Retweet the first tweet below if you can:
@ROKeefeMD @pointofcaremed This is exactly how I think about AKI! Great thread