
Ultimate Cardiac Thread for USMLE Step 2 CK - This thread will help you become a MONSTER at cardio on the NBME's / IM shelf / Family Med shelf
1) Long-QT syndrome --> implant cardiac defibrillator to prevent torsades! For family med shelf: advise patient not to play sports due to risk of sudden cardiac death
2) Easy point: FIXED, split S2 = ASD (atrial septal defect)
3) Teenager with asymptomatic murmur that isn't affected by preload/afterload exercises (aka inspiration or valsalva) Tx: NOTHING. *If it's holosystolic, diastolic murmur or congenital heart issues, this will require workup aka ECHO (the answer seems to always be ECHO lol)
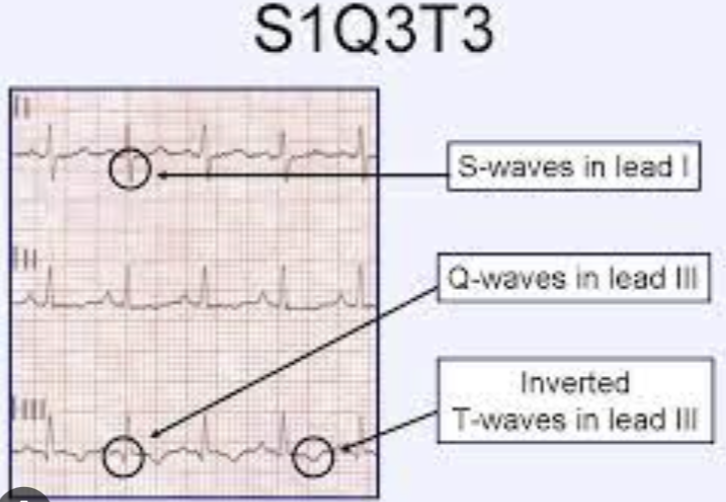
4) Chest pain + Decreased PCO2, decreased PO2, tachycardia, EKG with S1Q3T3 findings --> This is NOT cardiac in nature! These findings indicate a Pulmonary Embolism. Don't be fooled by the chest pain and EKG changes
5) Hepatojugular reflux & S3 or S4 = CHF Bout to drop some knowledge... Other conditions with hepatojugular reflux: - R sided heart unable to accomodate increased preload: a) CHF b) R sided infarct c) constrictive pericarditis d) restrictive cardiomyopathy
5a) NOTE: Cardiac Tamponade does NOT have increased hepatojugular reflux. Ez way to get tripped up **
6) SOB + Fever + HR > 100, Hypotension, perihilar fluid & cardiomegaly, decreased EF (usually 15-35% on questions) on ECHO = ACUTE MYOCARDITIS Question may give you coxsackievirus, parvo B19, doxorubicin usage, SLE/Sarcoid OR just a febrile illness as a clue
6a) Myocarditis can be mild or legit heart failure (USUALLY tested in a younger patient to show you it's not an acute coronary syndrome!) *Watch out for TQ saying "What is this condition associated with?" - Arrhythmias due to conduction disruption (may mention PVC's for example)
6b) Tx of Acute Myocarditis = supportive + tx underlying cause **Many students think that because of LOW EF in myocarditis question stems, they need to send patient to cath lab. This is wrong!
7) Acute Pericarditis = can ALSO be SOB + Fever, but EKG will show WIDESPREAD ST elevations & PR depressions! This is a money shot on your exam. Gotta know it. Pericarditis will usually have NORMAL EF bc it isn't affecting the myocardium
7a) Tx of Acute Pericarditis = anti-inflammatory meds (indomethacin, steroids or colchicine)
8) Constrictive Pericarditis = Chest pain that is WORSE with inspiration but BETTER with leaning forward --> Murmur will be coarse, sandpaper friction rub These patients will often have FEVER + hypotension + tachycardia too. So do NOT get thrown off. Look for key differences
8a) Summary of high yield differences: diastolic friction rub = constrictive pericarditis widespread ST elevation = acute pericarditis decreased EF = acute myocarditis **Chest Pain WORSE when lying down = pericarditis until proven otherwise (get's better with leaning forward)
9) Regular, narrow complex EKG, exacerbated by EtOH / nicotine / caffeine / stress = PSVT (paroxysmal supraventricular tachycardia) Tx: Vagal move (ice water over face, carotid sinus massage, coughing, valsalva) If vagals fail --> adenosine If UNSTABLE (low BP) = cardioversion
10) Murmur that is QUIETER with increased preload AND afterload = HOCM
11) Infective Endocarditis + New Murmur --> STAT REPEAT ECHO (likely has severe valvular damage)
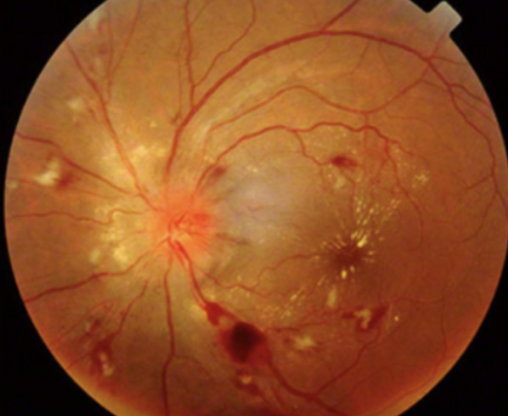
12) SEVERE HTN + Retinopathy: - retinal hemorrhage (seen below) - constricted retinal arterioles - lobular choroidal infarcts - hard exudates **LINEAR INNER RETINA HEMORRHAGES ARE SEEN IN HTN RETINOPATHY **Round hemorrhages of middle retina = diabetic retinopathy
13) BP Goal in adult < 140/90 BP goal in DM or CKD < 130/80 *They love this for Family Med Shelf
14) Test-taking tip: On the USMLE, don't pick slow ass scans like "radionuclide myocardial scan" or CTA, for patients in cardiac shock or having an MI! They're more useful for outpatient workup of angina / CAD
15) VSD can cause Failure to thrive! Look for a lil baby that fell off her weight/growth curve, SWEATS & FATIGUES during feeding + holosystolic murmur - Cause L to R shunt = increased PAH --> can reverse the shunt from R to L (Eisenmenger syndrome)
16) Which Glycogen Storage Disease has cardiomegaly + cardiomyopathy? POMPE! "it wrecks your PUMP" aka the heart
17) This TQ is worth bookmarking What has Kussmaul's sign? (impaired RV filling) - Restrictive cardiomyopathy - RV infarct - HUGE PE - Tricuspid stenosis - R sided CHF - Chronic constrictive pericarditis (tx: pericardiectomy) P.S. wtf is Kussmaul sign? JVD w/ inspiration
18) Treatment of cardiac tamponade - Pericardiocentesis! Watch for SBP decreasing 10mmHg during inspiration to dx aka pulsus paradoxus.
I had even more to add to this but Twitter wouldn’t let me make the thread any longer hahah Lmk if this helped! I can work on some for the other systems for the USMLE. - like/bookmark - retweet - drop a comment with any questions my friends!
If you wanna ace the surgery questions, check this thread out too 🥳🥳
Here’s a Heme/onc thread I put together using previously tested concepts: 🩸🧵🩸🧵
If you like this style of teaching & want to go through some high yields live, check this session out 👇👇 USMLE Step 2 CK - Top 20 TQ's to Know from NBME 12 in 2023 https://youtu.be/dbI3XtmhIKo
If you're a med student and would like to book a free call to discuss study strategy/classes/USMLE/COMLEX/rotations: https://www.actionpotentialmen...
JUST RECORDED THE CARDIAC STEP 2 / IM Shelf REVIEW! Subscribe on YouTube so you don’t miss it :) @ActionPotentialMentoring class="text-blue-500 hover:underline" target="_blank" rel="noopener noreferrer">https://youtube.com/@ActionPot...
GI REVIEW 💩💩🔥
The Cardiac Review is LIVE on YouTube! https://youtu.be/3LK-mudoRtE
@action_ap This was best
@Shifasheikh27 Thanks!!
@action_ap Thank you for this!
@smadad96 For sure! Thanks for dropping by and reading it :)
@action_ap Thank you!!
@Tomisin17132 Happy it’s useful for you!