
Surgery Shelf / Step 2 CK Cheat Sheet
1) Patient got some blood 2hrs ago + chills + fever = acute febrile non hemolytic transfusion rxn *This resolves on its own with Tylenol. Due to cytokines in the transfused blood itself To prevent this in the future, just give leukodepleted RBC's!
1a) Patient got blood + HEMOGLOBINURIA / Flank pain = hemolytic transfusion reaction due to ABO incompatibility
1b) Patient got blood 6hrs ago + SOB / lung crackles + EDEMA + elevated JVP --> Next step in management = CXR to evaluate for TACO (transfusion associated circulatory overload) tx: diuretics, sit upright, O2 via nasal cannula
2) UGI bleeding AFTER necrotizing pancreatitis + varices --> splenic vein thrombosis Pancreatitis inflammation causes splenic vein inflammation (it runs DIRECTLY on top of pancreas) Trick: Don't automatically go for CIRRHOSIS in questions with varices. Many med students do that
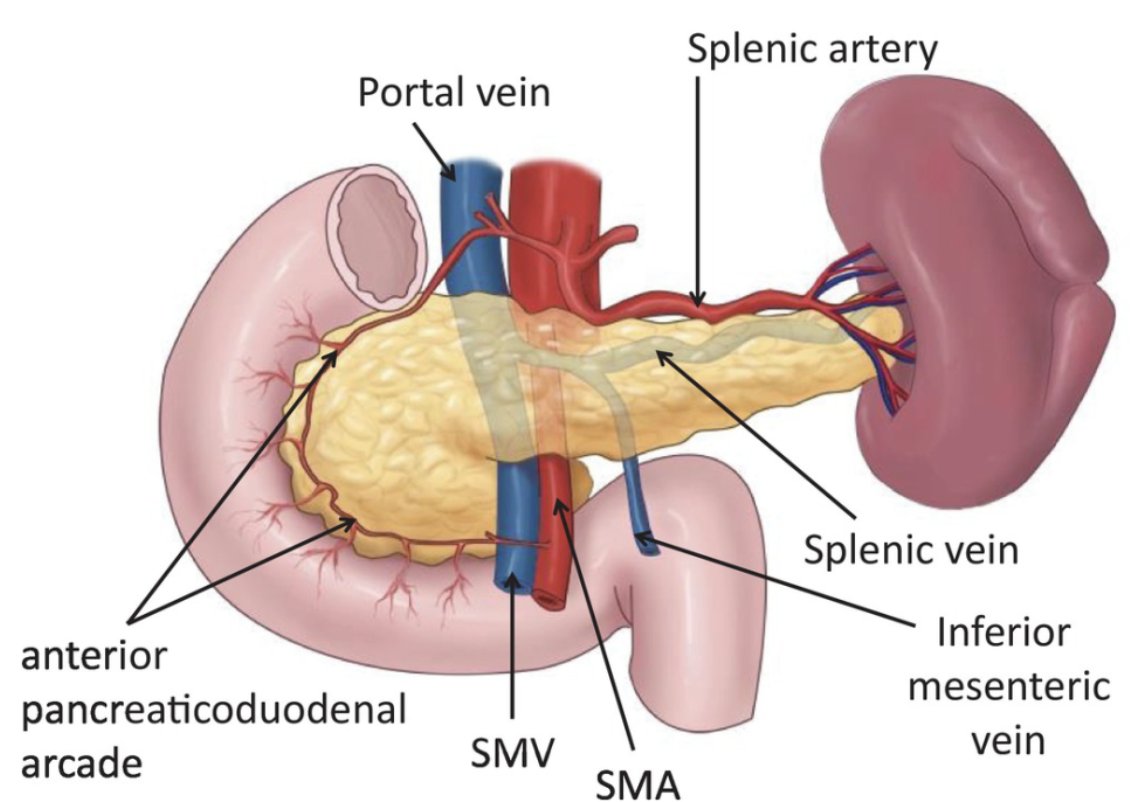
2a) Hepatic vein thrombosis aka Budd Chiari = would have hepatomegaly, portal HTN, jaundice, abdominal pain/distention
3) Cervical / thoracic spinal cord injury = shock + BRADYCARDIA (decreased sympathetic tone)
4) Hx that sounds like metastatic cancer + LBP/new Neuro sx's --> get an MRI of spine to eval for metastasis / caudal equine syndrome Cauda Equina - b/l LEX weakness, lose DTR/bowel/bladder, saddle anesthesia
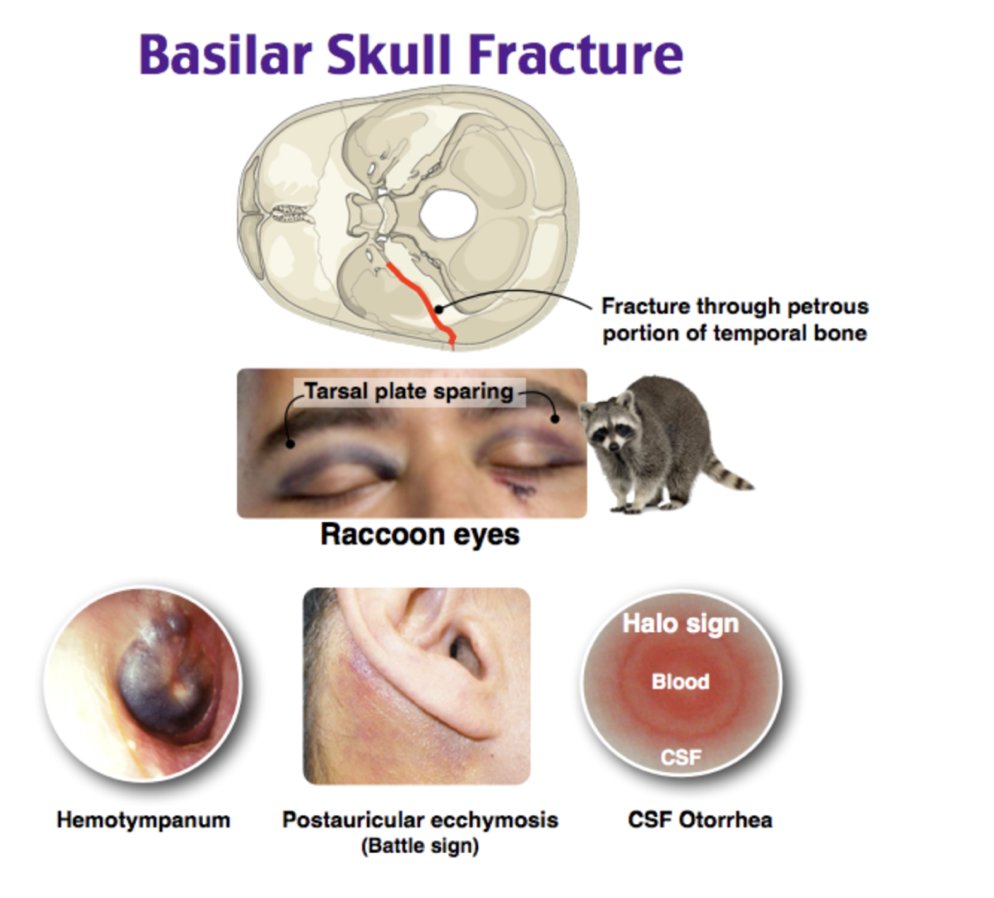
5) Head injury + clear fluid draining from ears = basilar skull fracture with CSF drainage (can also get CSF through nose via cribriform plate fracture)
6) Basal cell carcinoma with pathology showing tumor at margins --> best next step is reexcision of the excision site (EVEN if the incision appears well-healed!) *Do NOT watch and wait. Many students will get this wrong, assuming they can watch & wait for recurrence!*
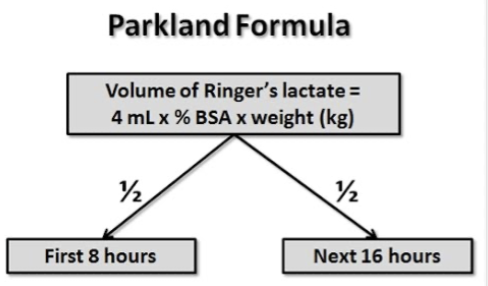
7) TONS of burns (> 20% BSA) = replace fluids ASAP
8) Benign sounding injury (scraped knee / hit elbow, etc in a diabetic) --> now with severe fever, crepitus at wound aka GAS IN TISSUES = necrotizing fasciitis Tx: immediate broad spectrum antibiotics (vanc/piperacillin + tazobactam + clindamycin) + fluids + surgery to excise
8a) Trick question with Necrotizing Fasciitis = you cannot waste time with an MRI! This is a clinical diagnosis (even tho an X-ray can help by showing gas in the tissues, it's not required)
9) Poor extension of wrist = radial nerve injury @ mid-shaft humerus
10) Post-op patient with HTN / Tachycardia + severe pain --> next best step is increase pain medicine to prevent pain-induced sympathetic tone causing HTN / tachycardia
11) Catheter-associated septic thrombophlebitis = fever + bacteremia + erythematous/indurated vein + drainage of pus from catheter Next step: broad spectrum IV antibiotics --> excision of vein Note: regular thrombophlebitis = elevate arm & warm/cool compress, NSAIDs
12) PE's can present with lungs clear to auscultation, no murmurs/gallops/no tenderness or edema of lower extremities! Don't let all of these negatives throw you off if the patient has a convincing history for a PE -cancer (cytokines = hyper coagulable) -dyspneic/tachy -postop
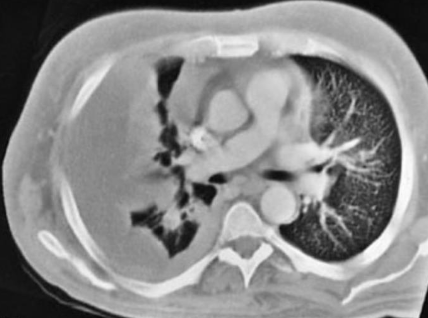
13) Liver transplant 2 months ago + SOB + fever + dullness to percussion of chest with this imaging finding = EMPYEMA After liver txp, you can get recurrent pleural effusions from inflam around R hemidiaphragm --> immunocompromised + bacteria = empyema Tx: chest tube + abx

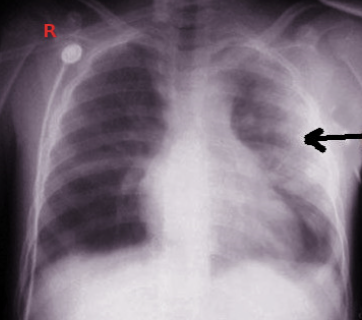
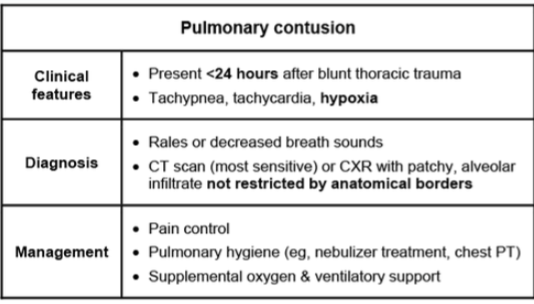
14) MVC + 24hrs later cough & crackles + afebrile = lung contusion
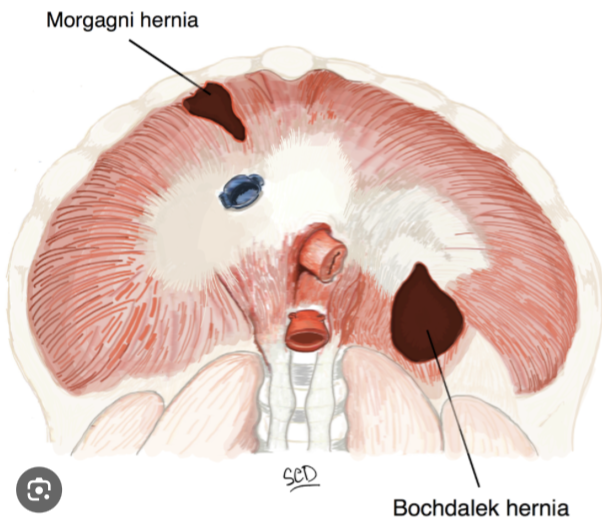
15) Xray showing obscured left hemidiaphragm and NG tube in lower left side of chest after MVC = diaphragmatic rupture **Important to know anatomy, this TQ is ALMOST ALWAYS in the back/left of the diaphragm!! (Bochdalek)

15a) On the other hand, Esophageal rupture presents as: - mediastinitis / crepitus over chest - fever - chest pain
16) ANC > 250 in ascites + abdominal pain/fever (usually an alcoholic & occurs out of nowhere) = Spontaneous Bacterial Peritonitis (SBP) Dx: Paracentesis w/ ANC > 250 Tx: 3rd gen ceps followed by ppx w/ Cipro or Bactrim
16a) Step 1 reminder: Pathogenesis of SBP: portal HTN causes bowel wall edema --> translocation of bacteria from gut
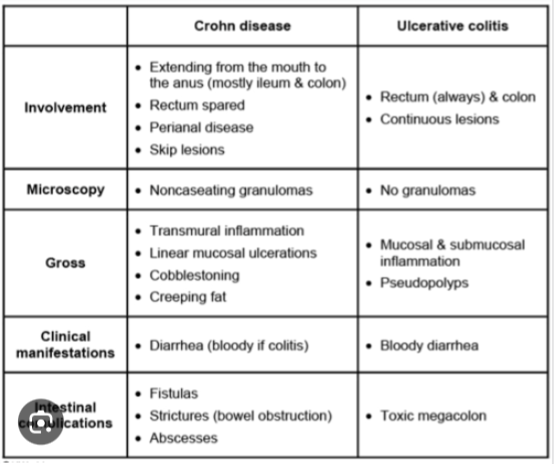
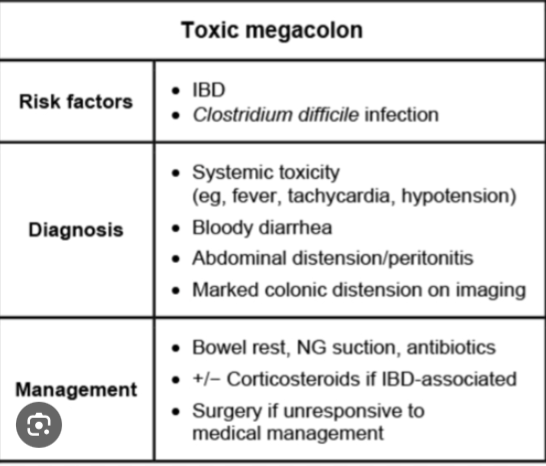
17) +ANCA & negative Saccharomyces cerevisiae Ab = Ulcerative Colitis Dx: colonoscopy Tx: rectum only = 5-ASA enema Extensive disease = oral 5-ASA + steroids. If refractory --> azathioprine/infliximab Refractory to everything or progression to toxic megacolon: total colectomy
I hope you enjoyed this Surgery Shelf / Step 2 CK High yield review! Don't forget to: - like/bookmark - retweet - lmk if there's any reviews you'd like to see next!
Excuse any typos lol I literally wrote this overnight from like 3-6am
There’s also a MASSIVE volume more of content I wanted to cover but Twitter’s thread length limit is stopping me haha Should I make a part 2??
If you're even remotely interested in our coaching program, feel free to check out our page. You can book a call with my team or I through this link --> Join here: https://www.actionpotentialmen...
JUST RECORDED THE SURGERY STEP 2 / SHELF REVIEW! Subscribe on YouTube so you don’t miss it :) @ActionPotentialMentoring class="text-blue-500 hover:underline" target="_blank" rel="noopener noreferrer">https://youtube.com/@ActionPot...
Surgery Crash Course review is on YouTube! Subscribe and share this vid with some friends to ace these TQ’s 💯🔪👇 https://youtu.be/TwLcNUNks5I