
Having an elevated Lp(a) increases your risk of heart disease. There are no currently approved therapies to Lp(a). But that doesn't mean you cannot lower your risk. Here's how 🧵👇 /1
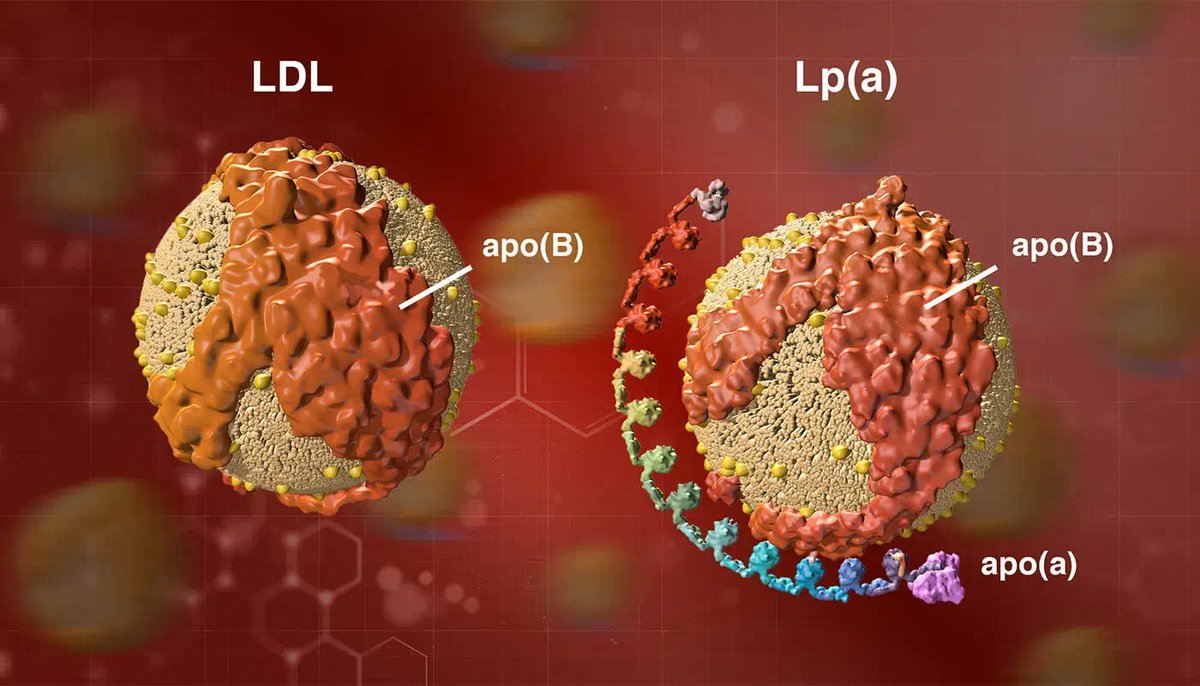
If you have an early family of heart disease, you need to assess your Lp(a) levels. Elevated Lp(a) is one of the most common genetic reasons people develop early heart disease. It is super common. In some populations, 20 - 30% of people have elevated levels of Lp(a). /2
But here’s the problem. Most people don’t know about it. Most doctors, even cardiologists, don’t test for it. There is at least a one in five chance I am taking about YOU. There is a 100% chance I am talking about someone you know. /3
This is a big problem, and we are doing too little about it. I have covered what Lp(a) is & why it is an independent risk factor for coronary artery disease In a previous article that you can find on my Substack "The most important heart test you've never heard of" /4
The big issue with having an elevated Lp(a) is that no approved therapy is currently available to lower it. And most people think that because there is no currently approved therapy to lower it that there is no way to reduce your risk because of it. I disagree. /5
Here’s how most people solve this problem: They ignore it. As Ayn Rand says: “We can ignore reality, but we cannot ignore the consequences of ignoring reality.” This is not a good strategy. /6
Here’s how the ‘Ignore It’ chain of logic goes. “There is no approved therapy to lower Lp(a) levels So why would I bother testing for it?”. Spoken like someone with absolutely no skin in the game in this instance. /7
There is indeed no currently approved therapy to specifically lower Lp(a) levels But that does not mean you cannot decrease a person’s risk. /8
Before we even get to ⬇️ risk in those with an ⬆️ Lp(a) I have a major criticism of the ‘not testing’ approach. Even if there wasn’t a way to lower risk We must OFFER people the opportunity to KNOW what might be causing their genetic risk of heart disease. /9
Who are we as doctors to say whether or not you should have an explanation? Maybe, just maybe, people might want to know, if even just for the sake of knowing. That might not be everyone’s desire, but it is for many patients I work with. /10
There are things you can do to lower your risk. Here’s how. Coronary artery disease is a multidimensional problem. Elevated Lp(a) levels are an important component in increasing that risk. /11
But many other things drive up risk Particularly if also in the presence of an elevated Lp(a). Metabolic Syndrome High Blood Pressure Inflammation Inactivity Smoking Diabetes We already have very effective lifestyle and drug therapy approaches to these problems. /12
For my patients who discover they have an elevated Lp(a) It has been the catalyst to start taking their lifestyle much more seriously As they can now see the penalty of not doing so. With this approach, we may not be lowering Lp(a) But we are reducing risk in total. /13
To date, there have been no reliable ways of integrating an Lp(a) result into a lifetime risk calculator. Until now. CAUSAL AI is an algorithm that calculates lifetime risk of a heart attack in those with ⬆️ Lp(a) & what ⬇️ LDL-C & ⬇️ Blood Pressure does to that risk. /14
Let’s take a 42-year-old male Who is a little overweight BMI 26.1 Has a systolic blood pressure of 130mmHg LDL-C of 4 mmol/L (155 mg/dl) And a family history of heart attack. This is what their risk of a heart attack out to age 80 looks like. /15
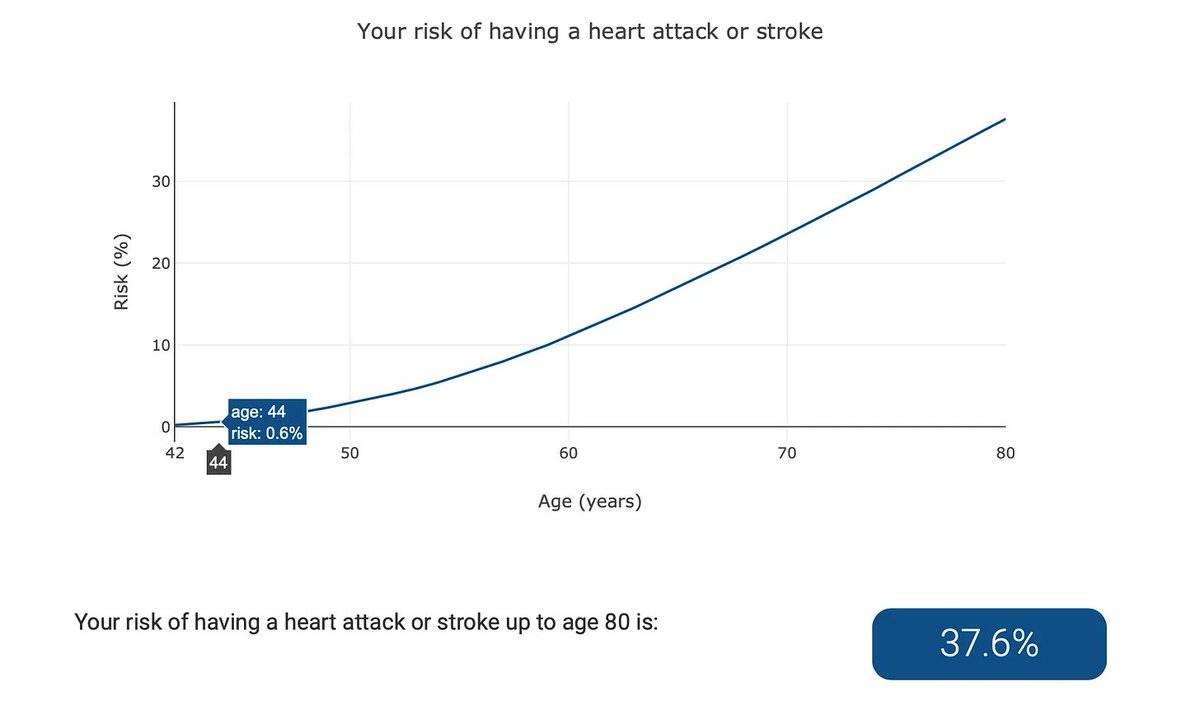
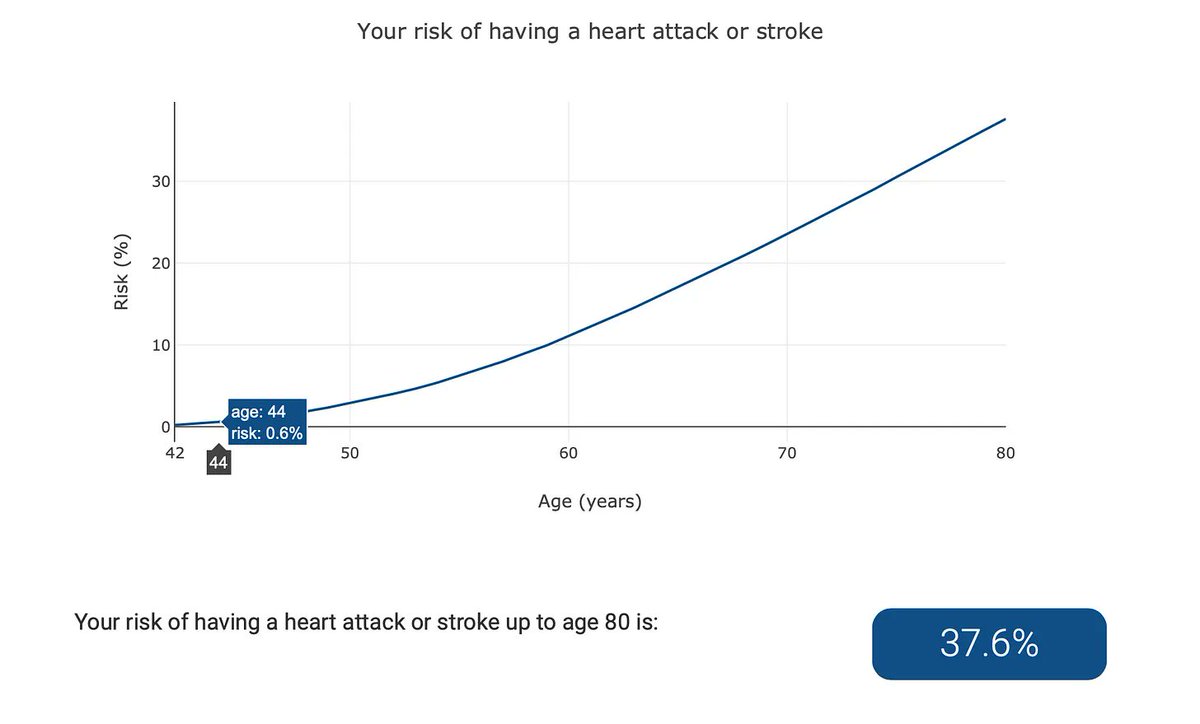
As you can see, the near-term risk is very low, in the sub-1 % range. However, the risk ratchets up fast. By age 60: 11% By age 70: 23% By age 80: 37% Now let’s see the same person’s risk if they have an elevated Lp(a). /16
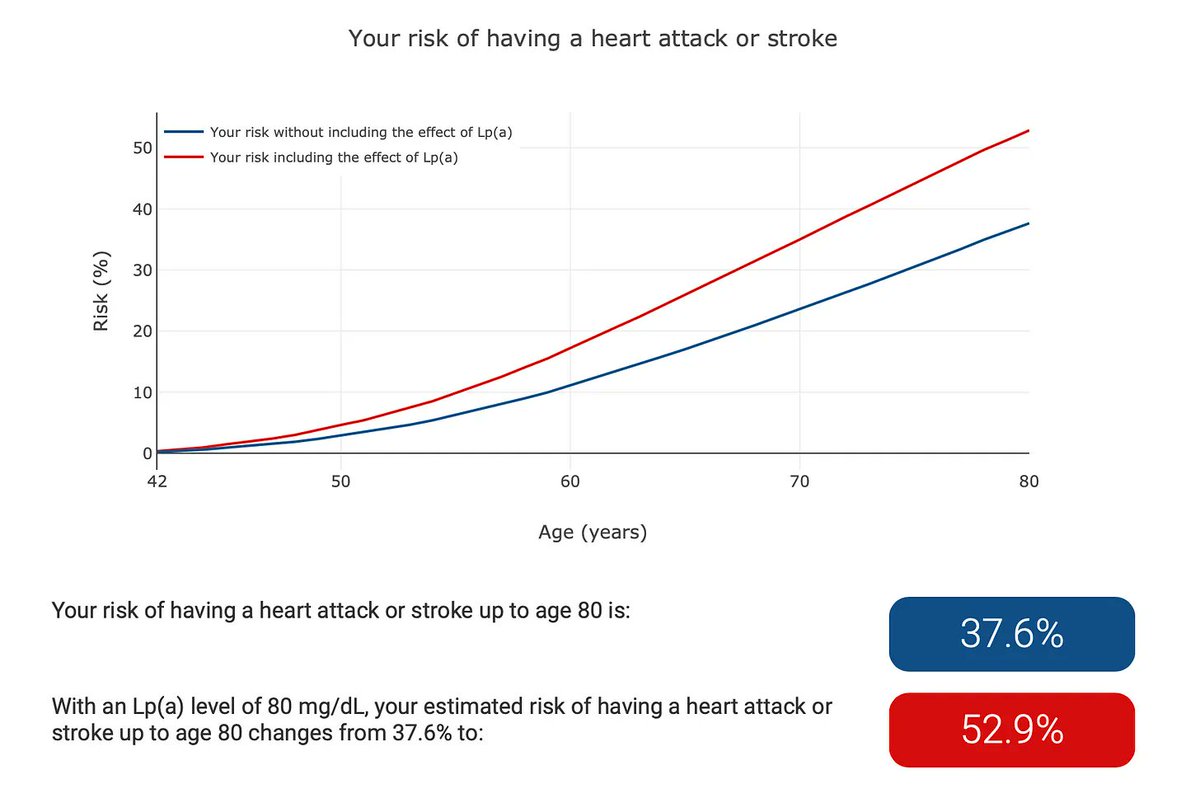
The red line indicates the real risk with the elevated Lp(a). See how things have changed. By age 60: 11% is now 17% By age 70: 23% is now 35% By age 80: 37% is now 53% Not measuring Lp(a) = Not accurately assessing risk. /17
Sure, knowing that you are at higher risk is useful, but it would be nice to see these figures go down. They can. Here’s how. By doing the simple things right regarding blood pressure and cholesterol management. /18
Let’s look at the same person with the elevated Lp(a) But now let’s reduce their LDL cholesterol by 2 mmol/l (77mg/dl) And their systolic blood pressure by 15 mmHg. Both are easy to do. The pale blue line is where we land. /19
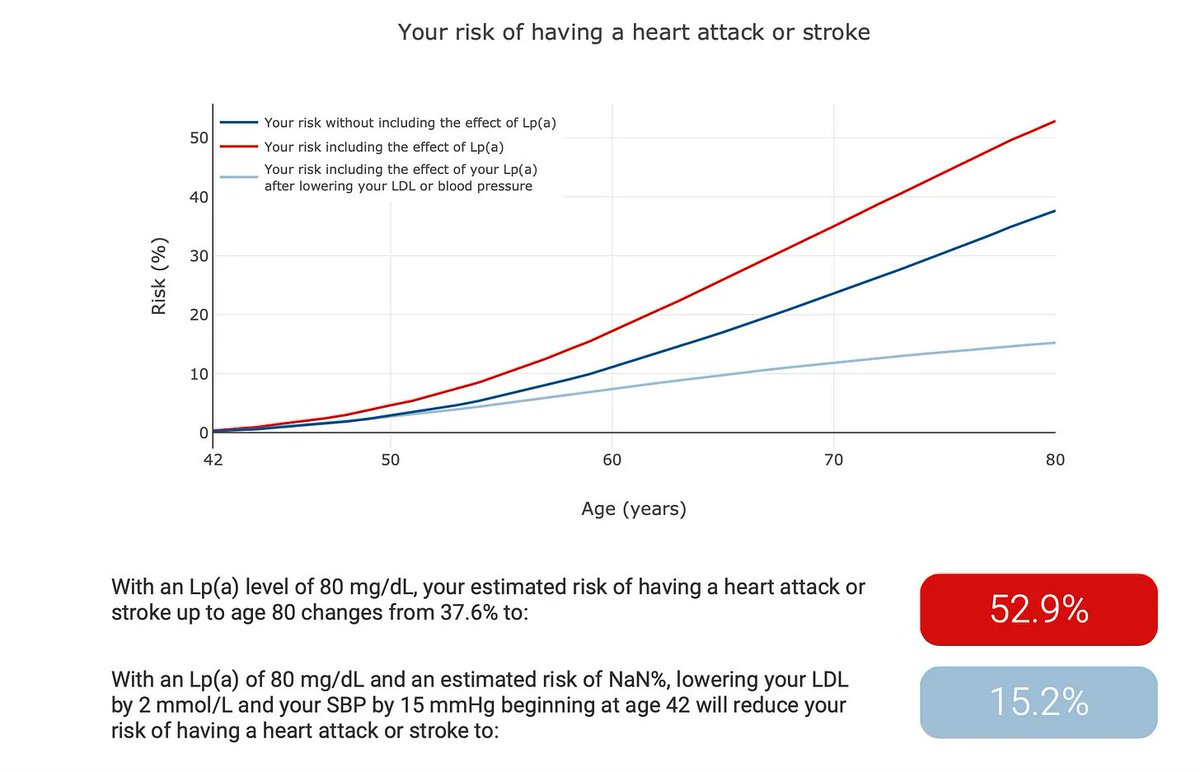
Once again, things are very different. By age 60: 17% is now 7% By age 70: 35% is now 12% By age 80: 53% is now 15% And this is WITHOUT lowering Lp(a)! So yes. There are no currently approved therapies to lower Lp(a). /20
But if anyone uses this as a justification for not testing for it, I would ask some serious questions. Always remember YOU have the most to win and the most to lose when it comes to cardiovascular risk. Only YOU get to decide what you think is high risk. /21
But you have to be dealing with at least accurate information to make that decision. Without knowing your Lp(a) levels, you are flying in the dark. /22
That's a wrap! If you want to check out the Lp(a) calculator, you can go to lpaclinicalguidance .com (Elon don't like links 😉) 👋 If you enjoyed this thread, then you will probably enjoy my free weekly newsletter. Link in my Bio above.
If you liked what you read here You will definitely enjoy my Free 5 Day Mini Course On Preventing Heart Disease. You can sign up for free here. https://www.drpaddybarrett.com...

@Paddy_Barrett Doc - this is helpful info to share but a terrible thread. Seriously urge you to rethink how you present a PoV.
@Paddy_Barrett @threadreaderapp unroll
@Paddy_Barrett Do you test for it in your Blackrock Clinic ?
@Paddy_Barrett Is there also a range to lp(a)? Like just having slightly elevated lp(a) vs very elevated? Or is it binary? Once it’s over 100 nmol/L it’s an issue?
@Paddy_Barrett How?
@Paddy_Barrett Lepodisiran
@Paddy_Barrett Is there any evidence that shows that lowering Lp(a) reduces CVD events? If so, could you please quote the source? Thanks