
There is one thing that, even as a reviewer and despite having pointed it out during the process, I really haven't understood about the new ESC guidelines for chronic coronary syndromes. Using the new Risk factor-weighted clinical likelihood (RF-CL) model, one can calculate

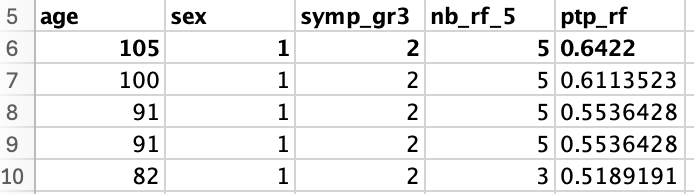
@DFCapodanno I think the reason is this: when calculating RF-CL, the upper age limit was set to 80. However, 0.6% of the dataset (a synthetic sample was provided in the supplement of the JACC paper, available at this link - https://vbn.aau.dk/files/33193... with 3061 patients) is older than 80 years.
@ihtanboga Thanks so much, you relieved my pain! The problem is that they indicate ICA for PTP>85%, but there is apparently no way to reach that score without risk enhancers, whose weight has not been quantified.
@DFCapodanno 4/Thus, classifying a patient into a high or very high likelihood category is based on clinical adjustments to the RF-CL estimate, NOT on any calculation.
@cvrints Thank you, Christiaan. Can we say then that if a patient has one of the risk enhancers his PTP goes straight to >85% (i.e., ICA)?
@DFCapodanno The prior model in 2019 actually was more simple and understandable. Patients and clinicians need simplicity in daily bust practice.
@DFCapodanno This very question was put out during the Q&A session with writing committee. The answer was vague and pointed us towards clinical sense to modify the risk based on additional factors that include CS and beyond. No concrete mechanism was presented… individuated approach.
@DFCapodanno Navigating the ESC Guidelines Maze: A Cardiologist's Conundrum 🧭❓ As a seasoned cardiologist with 15+ years in the field, I've seen my fair share of guidelines. But the latest ESC guidelines for chronic coronary syndromes have left even me scratching my head.

@DFCapodanno Thank you so much! I thought I was the only one who didn't understand!
@DFCapodanno Additionally, does somebody understand why a test is endorsed that places the majority of patients into the medium-risk class? Should a per-probability test's ability not be measured on how effective they are in "safely" ruling out patients, thus simplifying a physician's life?

@DFCapodanno Also, if I have interpreted correctly, isn’t it weird that someone with a very typical angina and no dyspnea only scores a 3 out of 5?
@DFCapodanno Preparing for a Talk about new ccs guidelines I asked myself the same question. Thank you for posting this. My conclusion are: 45%+ "I think he/she need ica" should do it... thanks to my clinical scills... (this is meant to be a joke...)
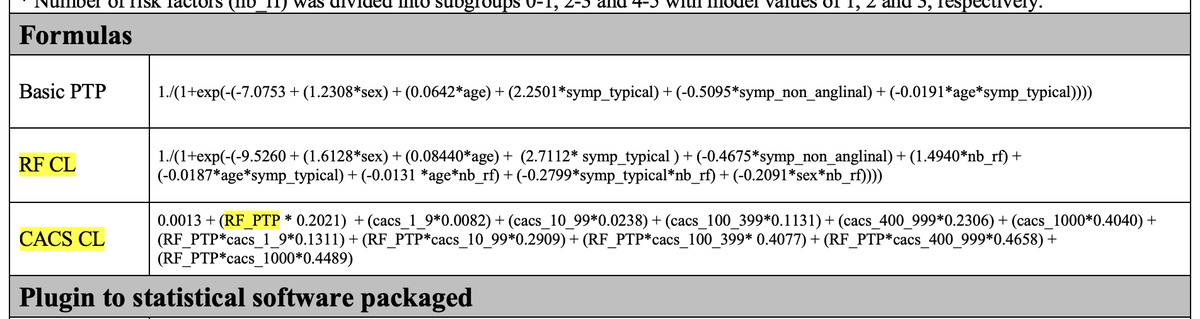
@DFCapodanno @DFCapodanno the supplementary material makes things clearer. two models. model 1 without the calcium score (max PTP 45%) Output of model 1 appears to be used as an input to model 2 along with the calcium score. model 2 results in a higher adjusted PTP. see formula.
@DFCapodanno 2/The 2024 GL expand on the concept of "clinical likelihood" introduced in the 2019 GL. According to this concept, the estimated pre-test RF-CL must be adjusted based on clinical data. Figure 5, part 2, lists several clinical factors that can increase or decrease this estimate.

@DFCapodanno I did not understand as well. CT is indicated when the pre test probability is between 5-50%. How could I choose the appropriate test if the maximum pretest probability is 45%? I did not find an on-line calculator.
@DFCapodanno Thank you!! 🙏 I also don‘t understand how to „correct“ the score. Add what number? Multiply with what?
@DFCapodanno 3/For instance, if a patient with a 45% pre-test likelihood shows severe symptoms during exercise, the clinical likelihood may exceed 85%. Similarly, segmental hypokinesia on echo may raise the likelihood above 45%.
@DFCapodanno 1/As you correctly pointed out, the maximum pre-test likelihood of obstructive CAD predicted by the risk factor-weighted clinical likelihood (RF-CL) model is 45% (moderate). In comparison, the highest pre-test probability in the basic PTP model from the 2019 guidelines was 52%
@DFCapodanno Did we ever get any more clarity on this? Or did it stick with - you get the result from the RF-CL - then make an educated guess of the added risk using the abnormal clinical findings they suggest?
@DFCapodanno I couldn’t agree more! It also sounds odd having to stop at just the calcium score when theoretically you could proceed with the CTCA for completeness and speed of decision making! Why stop, recalculate a score, then get another CTCA?! I this tool will be good to rule OUT than IN
@DFCapodanno My understanding is that no one qualifies for ICA based on age, symptoms and risk factors alone. I actually use this number (PTP) and have a n excel sheet to calculate the Bayesian post-test-probability after doing further testing, like stres-echo...