
🧵 Neuro-Sjögren’s: Beyond Dryness Sjögren’s Syndrome isn’t just sicca. When nerves get involved, it can be devastating — and often misdiagnosed. Here’s a deep dive into neurological manifestations of Sjögren’s Syndrome👇 #Rheumatology #NeuroSjögren #MedTwitter
1️⃣ How common is neuro involvement in Sjögren? 📊 ~20–30% of patients with primary Sjögren’s may develop neurological symptoms. It can precede dryness. It can mimic other diseases. That’s why it’s called a “great imitator.” Peripheral > Central nervous system involvement.
2️⃣ Peripheral Nervous System (PNS) Manifestations 🧠 The most common neurological feature. 🧩 Types: • Sensory ataxic neuropathy • Small fiber neuropathy • Mononeuritis multiplex • Cranial neuropathies (esp. CN V, VII) • Autonomic neuropathy • Trigeminal sensory

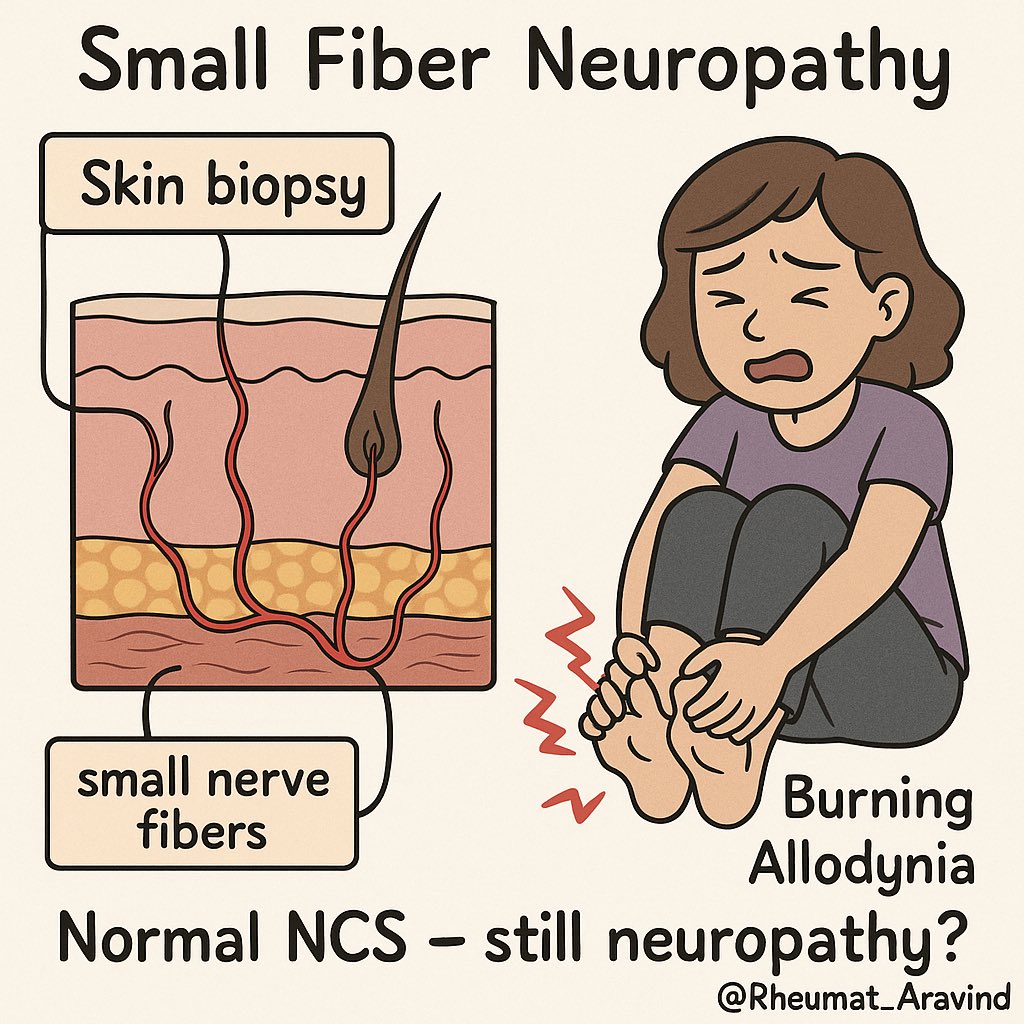
3️⃣ Small Fiber Neuropathy (SFN) 🔍 Often missed. Symptoms: • Burning pain • Dysesthesia • Allodynia • Normal NCS/EMG 📌 Confirmed with skin biopsy (↓ intraepidermal nerve fiber density) or QST. 🧠 Strongly associated with fatigue and autonomic dysfunction.
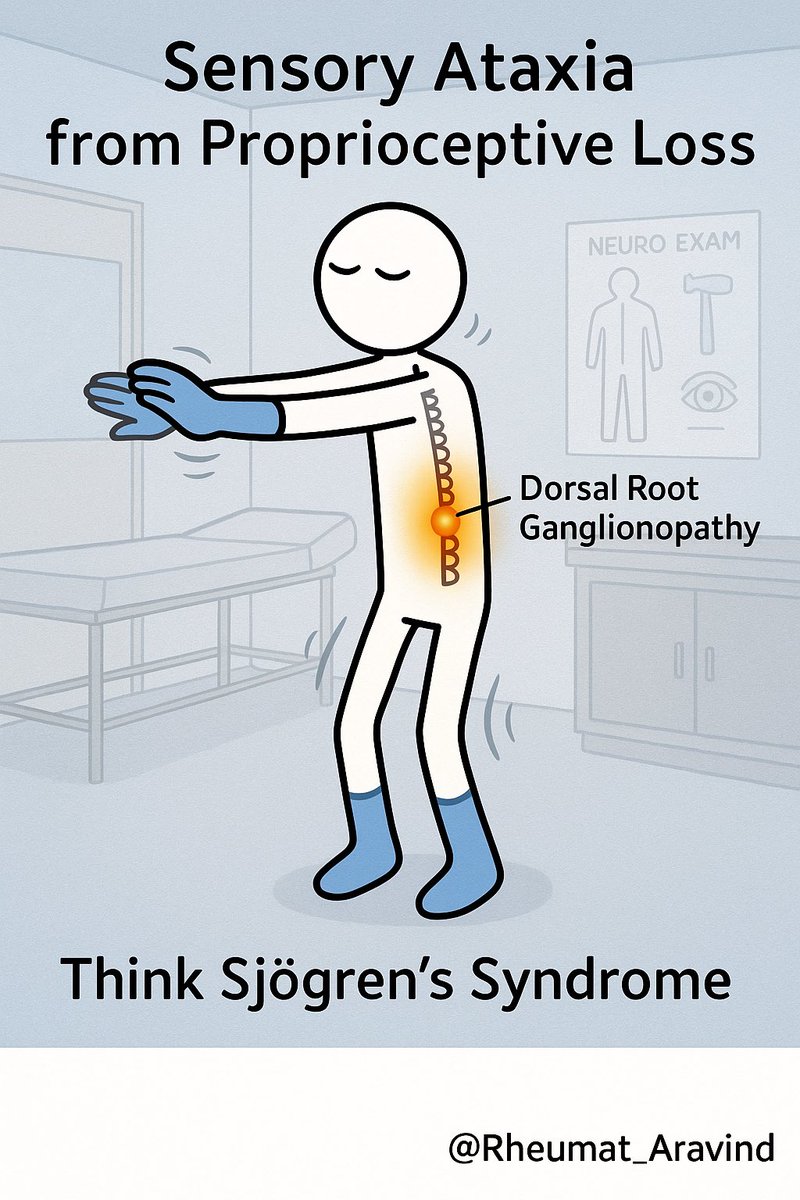
4️⃣ Sensory Ataxic Neuropathy 🎯 Most specific for Sjögren. • Loss of proprioception • Positive Romberg sign • Falls, imbalance • Normal motor strength MRI may show dorsal root ganglia enhancement. 🧪 May be the presenting symptom of primary Sjögren.
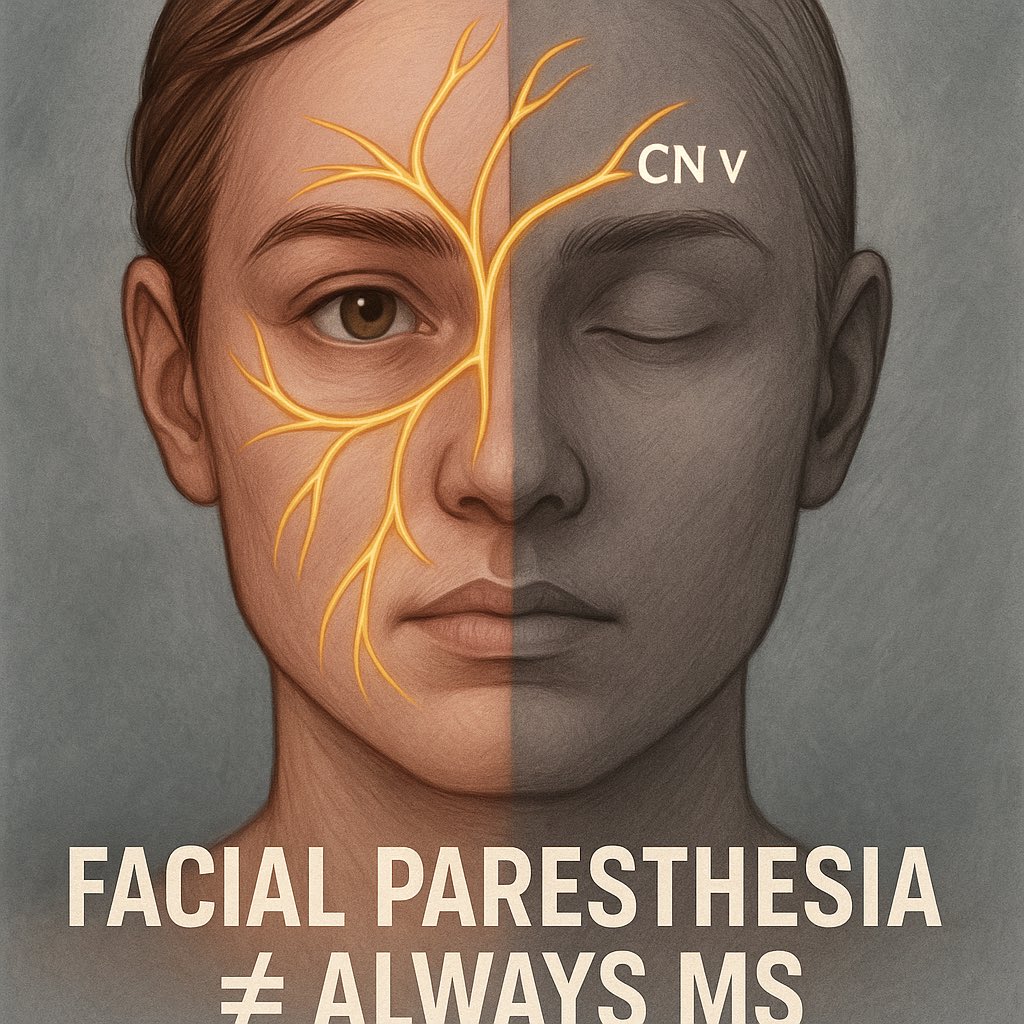
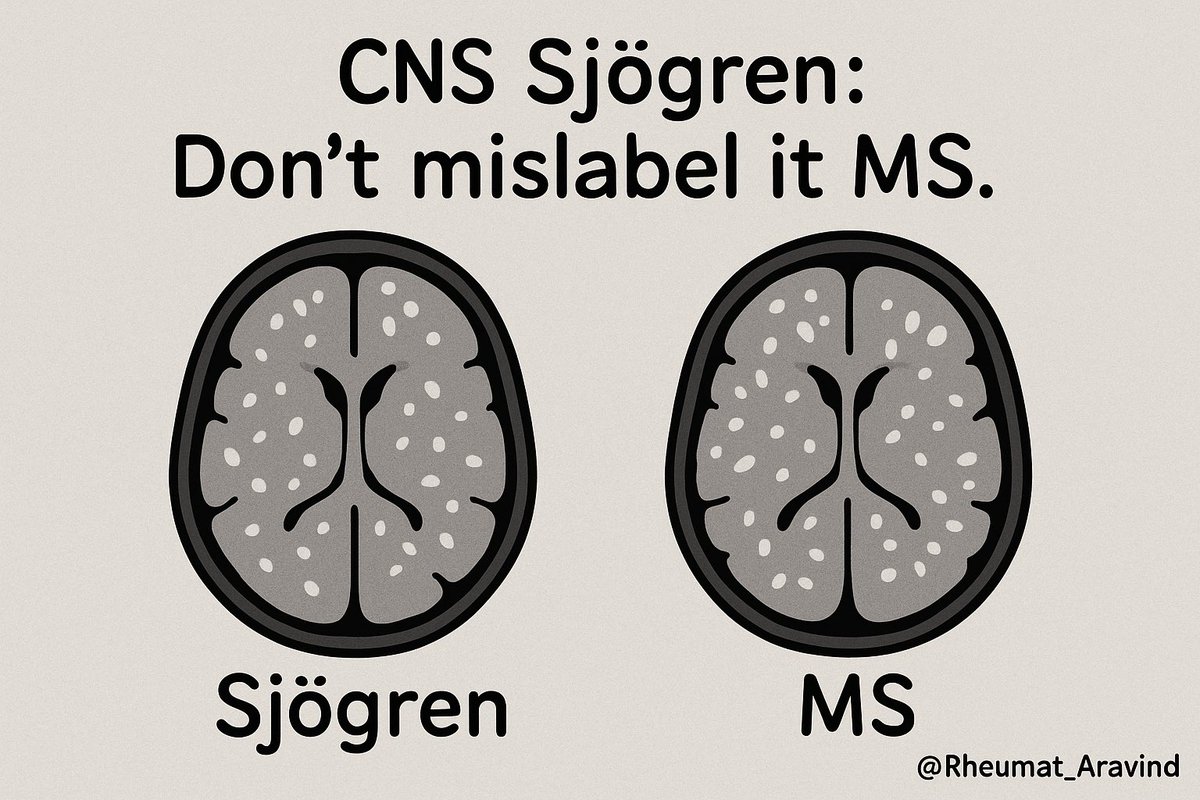
5️⃣ Trigeminal Neuropathy (CN V) 📍 Presents as facial numbness or paresthesia. Bilateral or unilateral. ⚠️ Often misdiagnosed as MS, especially if MRI shows nonspecific white matter lesions. Red flag = demyelinating mimicry in Sjögren.
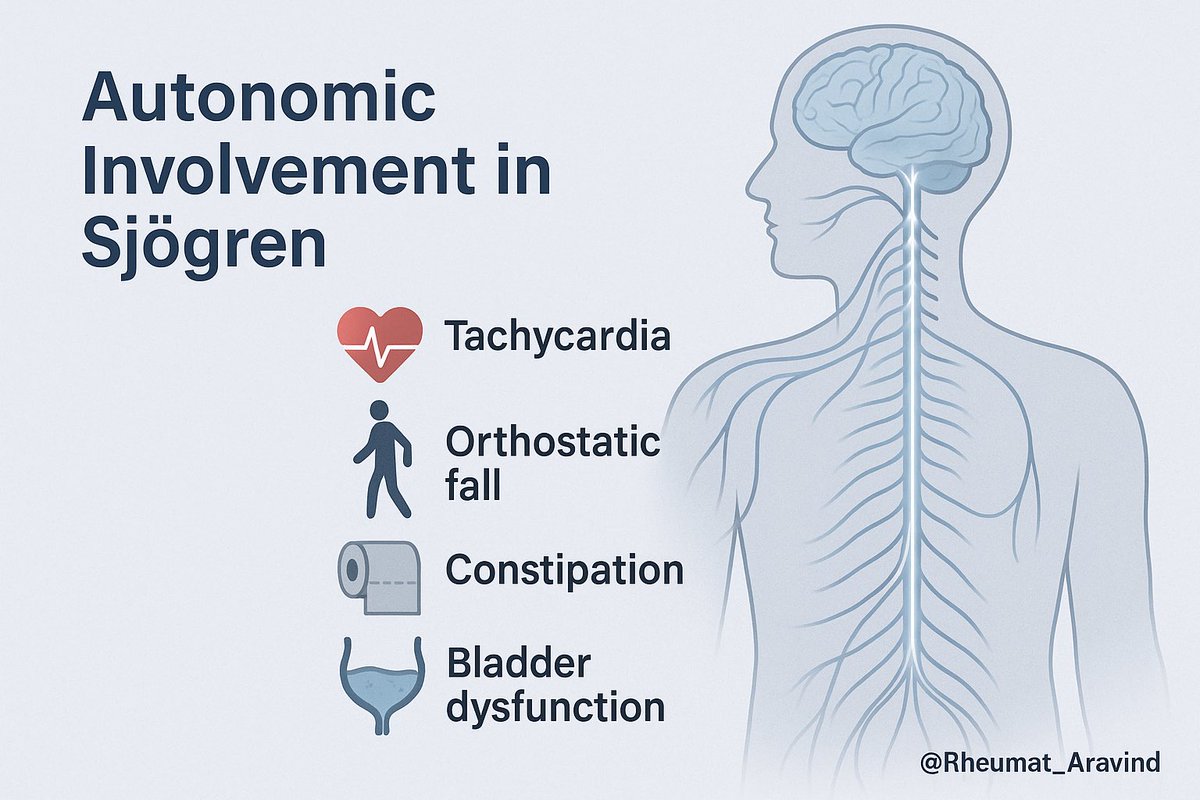
6️⃣ Autonomic Neuropathy 🌀 Affects: • BP regulation → orthostatic hypotension • GI motility • Bladder function • Heart rate variability Often overlaps with POTS or SFN. 🩺 Requires autonomic testing (HRV, QSART).
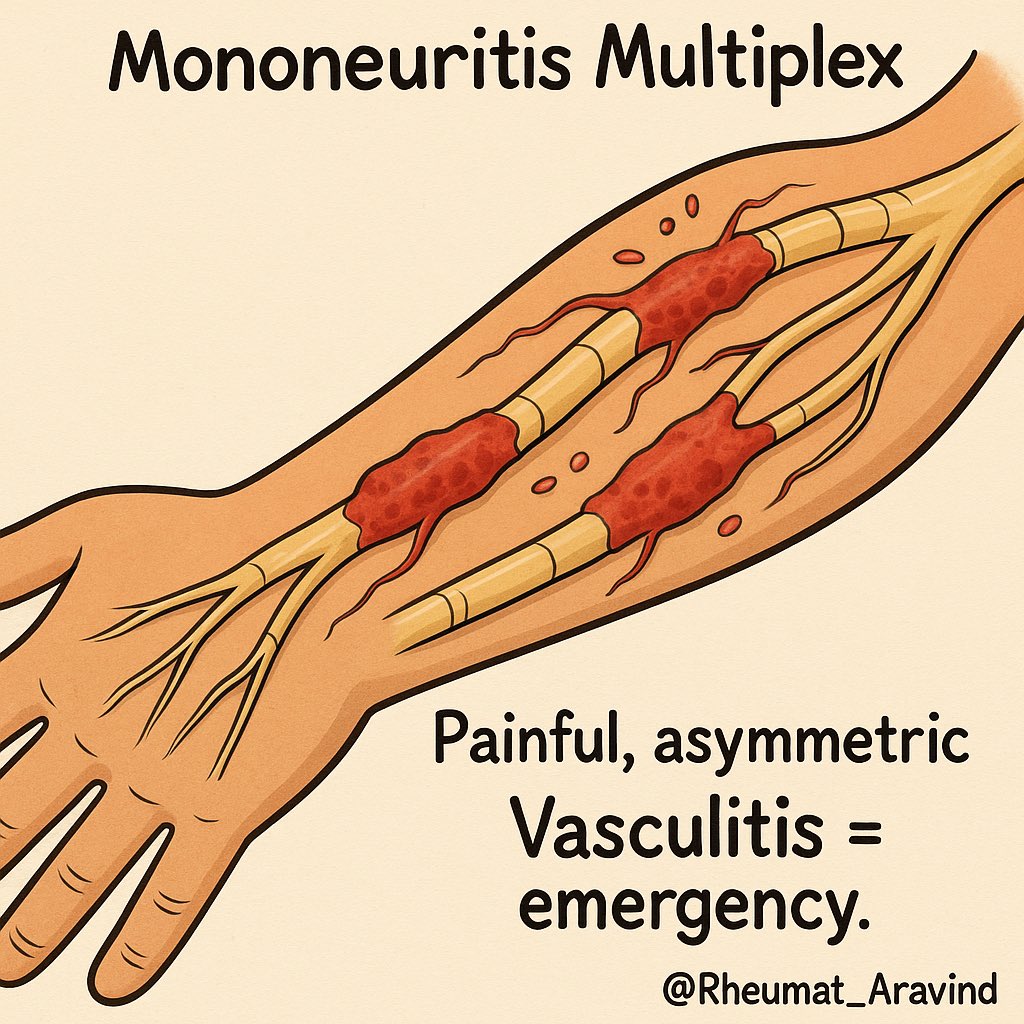
7️⃣ Mononeuritis Multiplex ⛔ Acute, painful, asymmetric neuropathy. Often due to vasculitis of vasa nervorum. Check: • ESR, CRP • Cryoglobulins • Complement levels • Nerve biopsy if needed Treat aggressively — this is organ-threatening.
8️⃣ CNS Involvement in Sjögren Less common, but serious. 🧠 Can resemble: • MS • NMO spectrum disorders (anti-AQP4) • ADEM • Cerebral vasculitis • Transverse myelitis • Cognitive dysfunction (“brain fog”) ⚠️ Demyelinating lesions + sicca = screen for Sjögren!
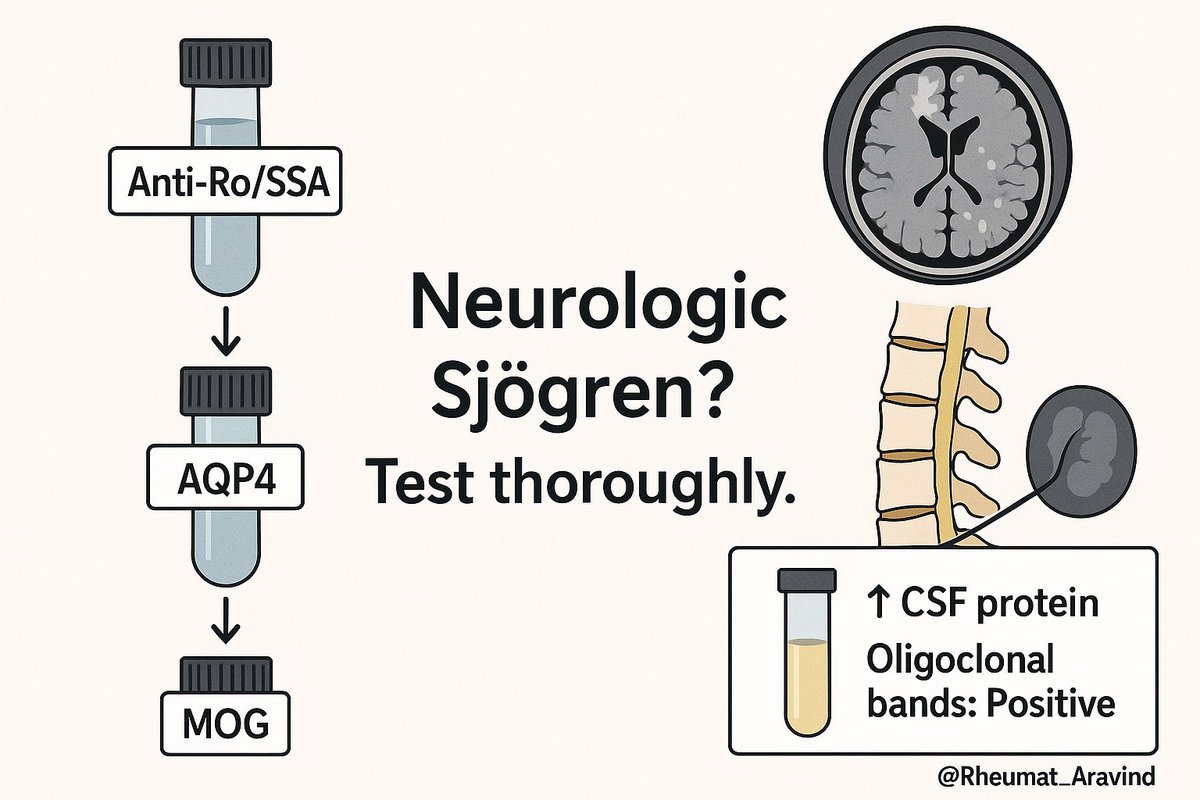
9️⃣ Anti-Ro antibodies and CNS Sjögren 💡 Anti-Ro/SSA often positive, but not always. Anti-AQP4 and MOG should be tested in myelitis or optic neuritis. CSF: • Mild lymphocytosis • ↑ protein • Oligoclonal bands (can mimic MS)
🔟 Neuropsychiatric & Cognitive Involvement 🧠 “Brain fog” is real. Can manifest as: • Memory issues • Difficulty concentrating • Depression • Anxiety PET scans may show hypometabolism in frontal/temporal lobes. 🧠 Mechanism: chronic inflammation + cytokines.

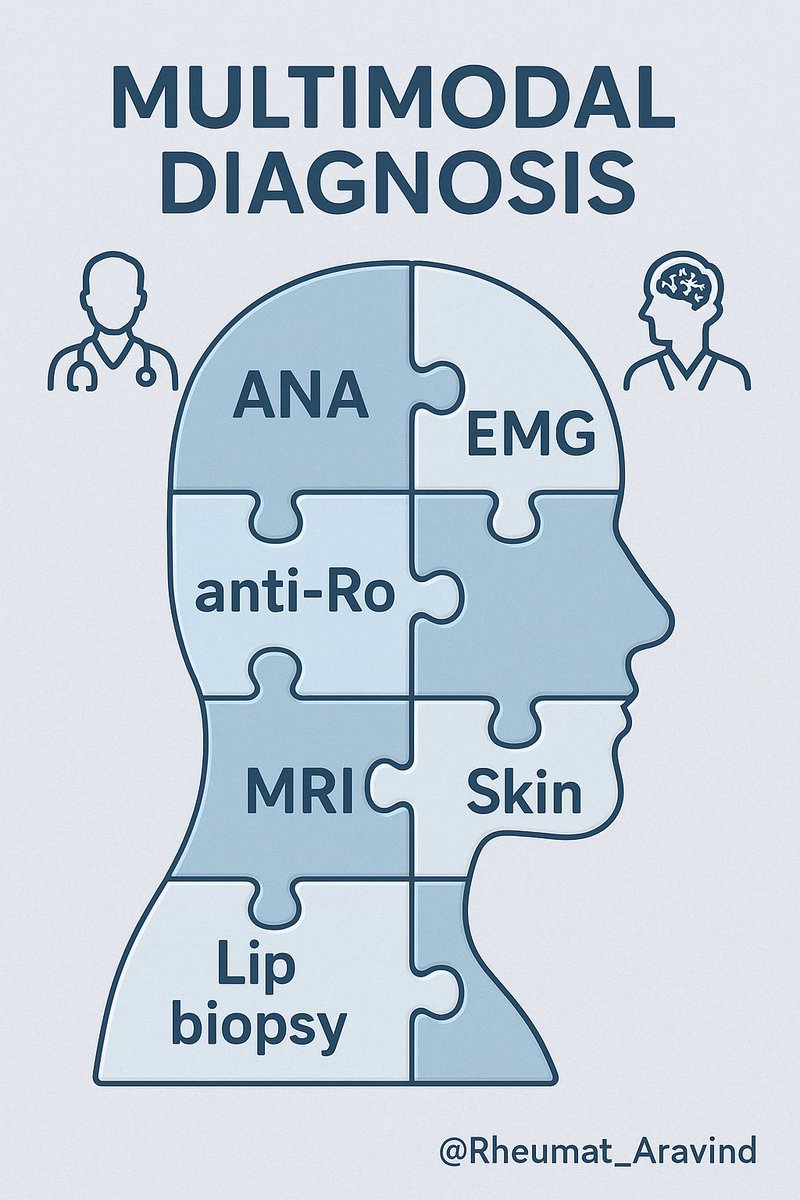
1️⃣1️⃣ Diagnosis of Neuro-Sjögren 🧪 Workup: • ANA, anti-Ro/SSA, anti-La/SSB • Cryoglobulins, complements • Lip biopsy (focus score ≥1) • Schirmer’s, salivary USG • NCS/EMG, skin biopsy, MRI brain/spine 🧠 Often needs multidisciplinary input — neurology + rheumatology.
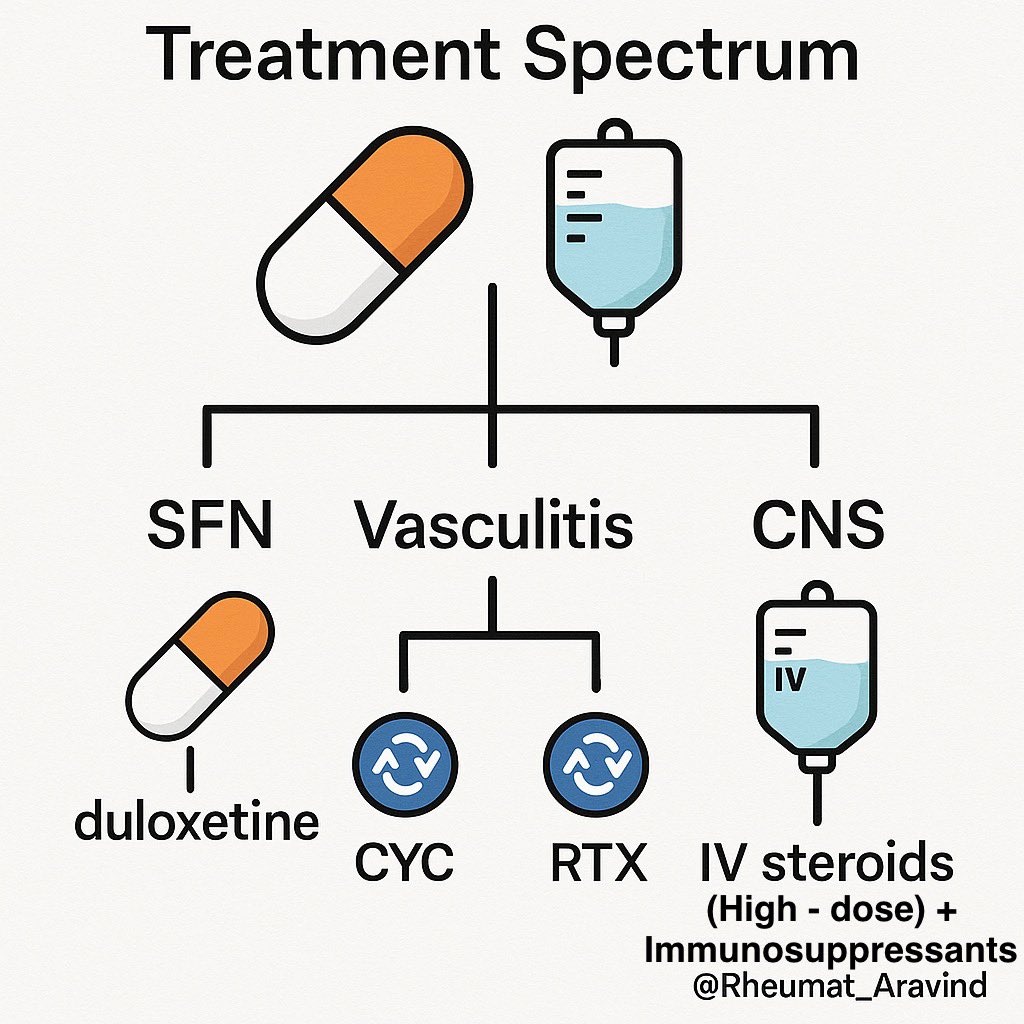
1️⃣2️⃣ Treatment Principles Depends on phenotype: ✔️ SFN / mild sensory – Gabapentinoids, duloxetine, IVIG (in select cases) ✔️ Mononeuritis multiplex / vasculitic neuropathy – Steroids + cyclophosphamide or rituximab ✔️ CNS involvement – High-dose steroids, immunosuppressants
1️⃣3️⃣ Prognosis ✴️ Early recognition = better outcomes. ✴️ Delay can lead to permanent damage — esp. in dorsal root ganglionopathy. ✴️ Autonomic and small fiber neuropathy may persist despite treatment. Don’t wait for dryness. Think Sjögren early.

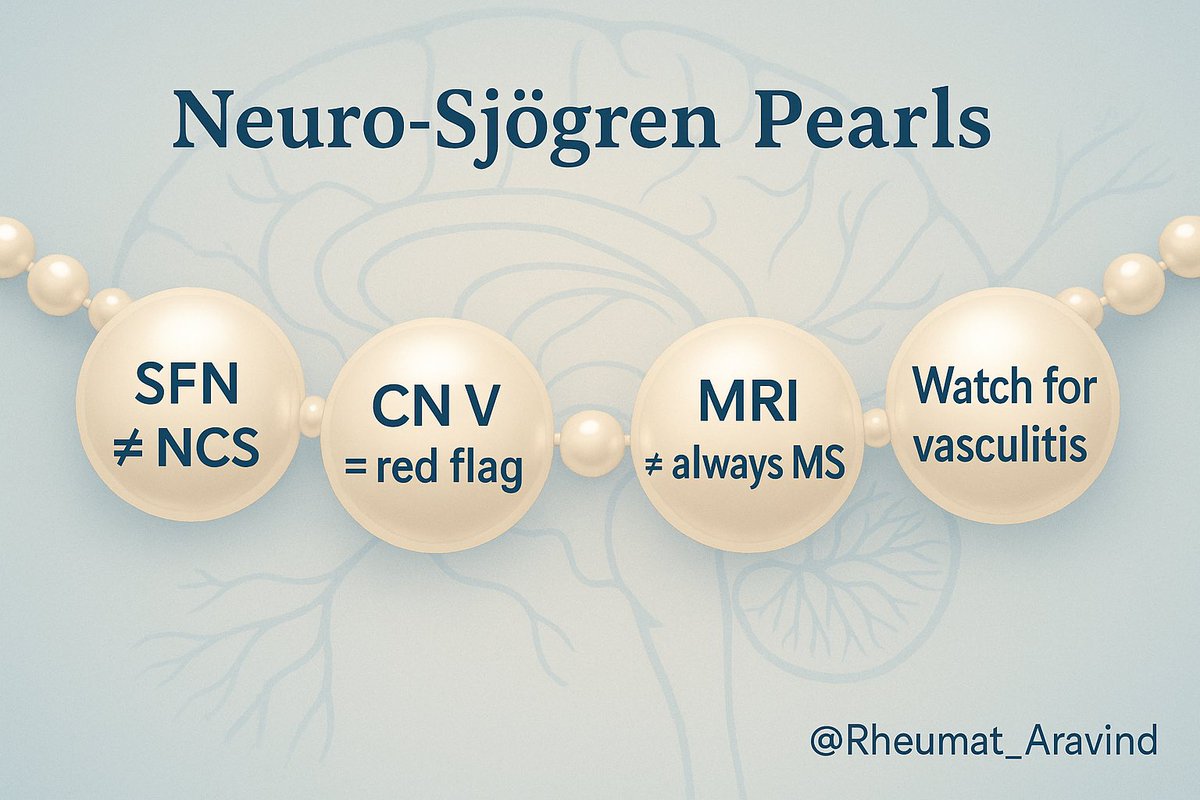
📍Key Clinical Pearls • Neuro symptoms may precede dryness. • SFN = common + often overlooked • Trigeminal neuropathy is a red flag. • CNS Sjögren can mimic MS/NMO • Skin biopsy can be diagnostic when NCS is normal • Always treat vasculitic forms aggressively.
🙏 Thanks for reading! Neuro-Sjögren is underdiagnosed, often misunderstood, and yet profoundly disabling. If you see a patient with unexplained neuropathy, don’t forget to screen for Sjögren’s — even if dryness isn’t the headline. #NeuroSjögren #RheumTwitter #SjögrensSyndrome

Skin biopsy ≠ rule-out SFN SFN can be clinically diagnosed Will work on a thread for neuro-APS soon.