
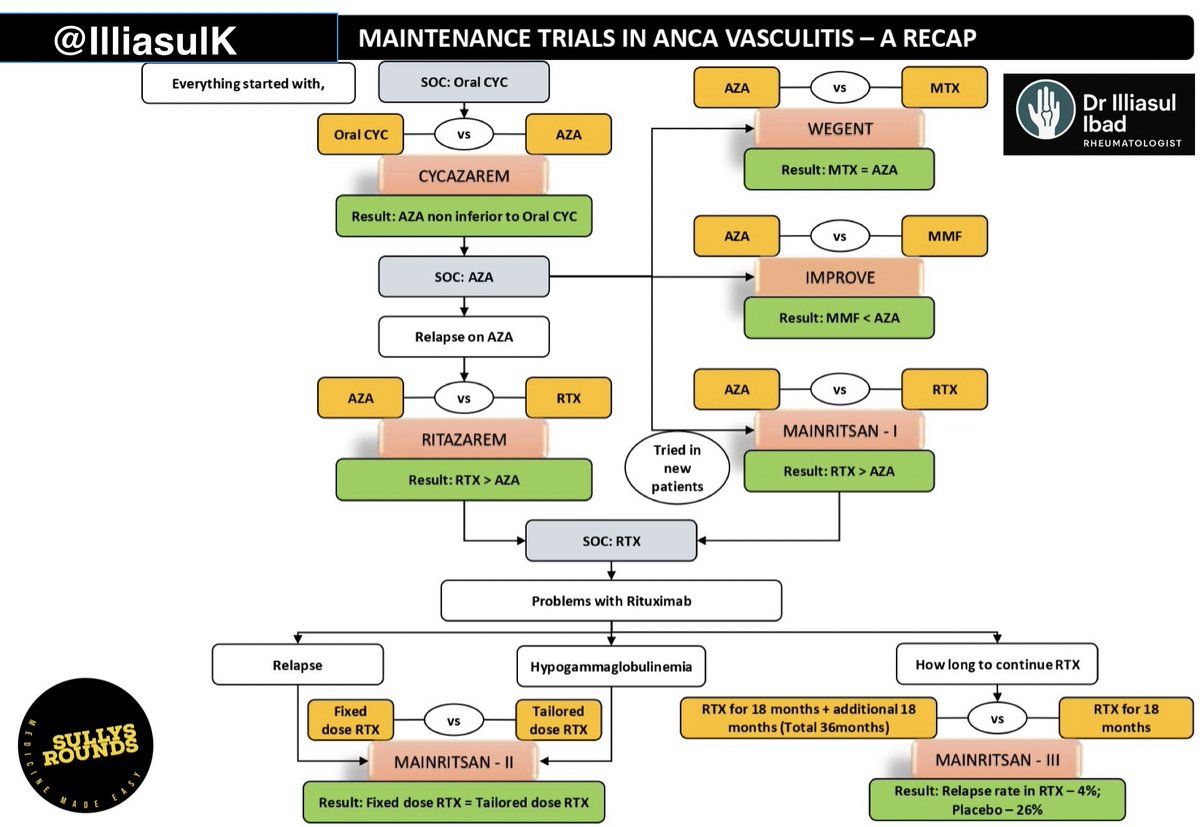
🧵How Clinical Trials Revolutionized ANCA Vasculitis Maintenance 💥 From cyclophosphamide to rituximab — this is the journey of evidence, one trial at a time. 🔁 Facts. Timelines. Game-changers. 📚 A must-read for every physician, rheumatologist, nephrologist, pulmonologist &

1/ 📍Why we needed trials In the 90s, patients with ANCA vasculitis had to stay on oral cyclophosphamide (CYC) even after remission. 🧨 Yes, it worked — but came with… • Infections • Infertility • Cancer risks We needed safer maintenance options. Let’s see what trials found

2/ 🔬 CYCAZAREM Trial (NEJM 2003) ❓ Could AZA replace oral CYC after remission? PICOT: P – AAV patients post-CYC induction I – Azathioprine C – Oral Cyclophosphamide O – Relapse T – 18 months ✅ Conclusion: AZA = CYC in efficacy, with fewer side effects. → AZA became
3/ 🔬 WEGENT Trial (NEJM 2008) ❓ Could Methotrexate (MTX) be as good as AZA? PICOT: P – AAV in remission I – MTX C – AZA O – Relapse + AE T – 24 months ⚖️ Conclusion: MTX ≈ AZA in low-risk patients. → MTX was a valid alternative, especially in non-severe disease.
4/ 🔬 IMPROVE Trial (JASN 2010) ❓ Could Mycophenolate Mofetil (MMF) replace AZA? PICOT: P – AAV post-remission I – MMF C – AZA O – Relapse free survival ❌ Conclusion: MMF had significantly higher relapse rates. → MMF fell out of favor for routine maintenance.
5/ 🔬 REMAIN Trial (Rheumatology 2017) ❓ Should AZA be given for 24 or 48 months? PICOT: P – AAV in sustained remission I – AZA for 48 months C – AZA for 24 months O – Relapse T – 48 months ✅ Conclusion: Longer AZA reduced relapse (22% vs 63%) → Extended AZA to 48 months
6/ 🔬 MAINRITSAN-1 (NEJM 2014) ❓ Is RTX better than AZA for maintenance? PICOT: P – AAV post-induction I – RTX (500 mg ×2 then q6mo) C – AZA O – Major relapse T – 28 months ✅ Conclusion: RTX had 5% relapse vs 29% with AZA. → RTX > AZA for maintenance.
7/ 🔬 MAINRITSAN-2 (ARD 2018) ❓ Can we tailor RTX dosing based on ANCA/B-cells? PICOT: P – AAV in remission I – Biomarker-driven RTX C – Fixed RTX O – Relapse T – 28 months ⚖️ Conclusion: Similar outcomes. Tailored RTX needed fewer infusions, but slightly more relapses.
8/ 🔬 MAINRITSAN-3 (ARD 2020) ❓ Should we extend RTX to 36 months vs stopping at 18 months? PICOT: P – AAV in remission I – RTX for 36 months C – RTX for 18 months O – Relapse T – 28 months (primary endpoint) after completing 18 months of RItuximab as per MAINRITSAN 2 ✅
9/ 🔬 RITAZAREM Trial (ARD 2023) ❓ What’s best in patients who relapse — RTX or AZA for maintenance after re-induction? PICOT: P – Relapsing AAV post-RTX induction I – RTX (1000 mg q4mo ×5 doses) C – AZA O – Time to Relapse ✅ Conclusion: RTX significantly better at
Ever tired of memorizing ANCA vasculitis trials? Here’s the story behind the studies—not just names, but logic, thought process, and how each trial shaped clinical reasoning. 📖 Read. 💭 Reflect. 🔁 Repurpose. 🧬 Maintenance in ANCA Vasculitis evolved like this: CYC → AZA →
@IlliasulK @threadreaderapp unroll
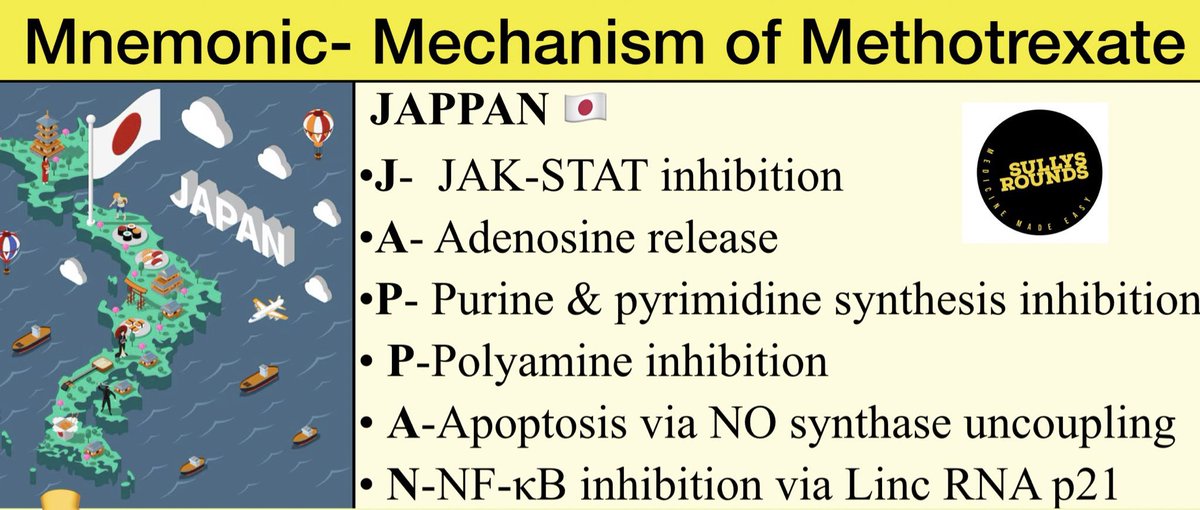
❓Is Methotrexate just a folate antagonist? Not at all—it’s much more powerful (and tricky). 🇯🇵 JAPPAN mnemonic: J → JAK-STAT 🚫 A → Adenosine ↑ P → Purine/Pyrimidine 🚫 P → Polyamine 🚫 A → Apoptosis via NO N → NF-κB 🚫 ⚔️ Side effects – 2 faces of MTX: • Anti-folate
🧵 Masterclass Highlight | #VasculitisConclave Jaipur A brilliant session by Dr. Pui Y. Lee on diagnosing DADA2 (Deficiency of ADA2)—a rare, monogenic vasculitis. ⚒️ADA2 residual activity does NOT correlate with disease activity 🌄A 25% cutoff detects ~90% of cases 🧪 ⚓Anti TNF



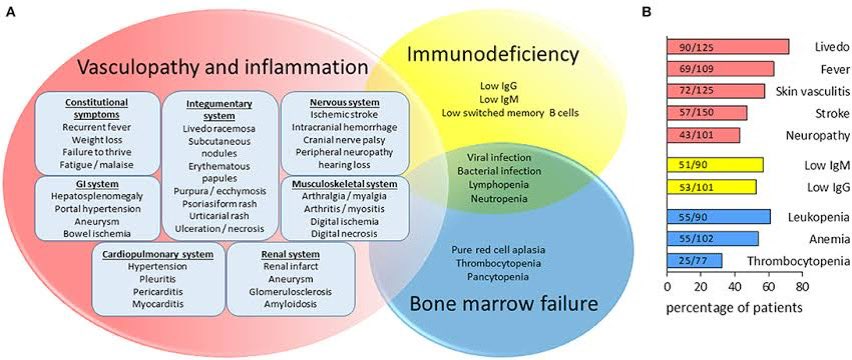
Title: Insights from Vasculitis Conclave 2025 •Genetic Susceptibility: Vasculitis tied to FCGR2A (1q23.3), IL1B (6q33.3), IL10 (1q32.1) for TAK, BD, KD. #Vasculitis #Genetics •ADA2 Deficiency: Leads to vasculopathy, immunodeficiency, bone marrow failure; low IgG/IgM,


"Spiked Helmet Sign" (SHS). A. This ECG tracing shows the characteristic "dome and spike" pattern of the SHS, particularly evident in the inferior leads (II, III, aVF), where the arrows point to the elevated and peaked ST segments resembling a spiked helmet.
