
🩸Hematology for The Non-Hematologist🩸 (A practical educational series for internal medicine trainees and physicians) Episode 8: 📞 “Doc, patient’s WBC just came back at 150,000 with majority blasts…” 👉🏻 here’s what you need to know about acute myeloid leukemia (AML)
Disclaimer: This thread is for educational purposes only and is not medical advice. Always consult hematology and medical oncology or appropriate specialists for patient-specific decisions.
1/ A 75-year-old man walks in looking exhausted. He says he’s been feeling “run down” for the past 3 days. What really worried him wasn’t the fatigue it was that his gums started bleeding when he brushed his teeth, and he’s noticed new bruises popping up on his arms and legs. “I
2/ Acute Myeloid Leukemia (AML) is one of the true emergencies in hematology. The reality is, these patients can crash fast, hours, not days. ⏳ Hyperleukocytosis, DIC, infection, tumor lysis… all of them can hit at once. This is not a solo job. It takes the ED, ICU, internal
3/ So what actually is AML? Remember what we said last week: – Acute = disease of immature cells, presenting fast and aggressive. – Myeloid = cells from the myeloid lineage (granulocytes, monocytes, platelets, RBC precursors). – Leukemia = cancer in the bone marrow and blood,
4/ “What clinical picture should make me suspect AML? 🧐” These are the symptoms that should make you reflexively think of acute leukemia. On their own, some may look nonspecific. But when they cluster together, they’re a red flag 🚩🚩🚩🚩 Think about it as bone marrow
5/ Your CBC is usually the first clue. See a white count of 150k? 🚨 Think acute leukemia. But here’s the twist: acute leukemia can also present with leukopenia. So don’t let a low WBC lull you into thinking you’re out of the woods. 💡 Why can AML present with leukopenia?
6/ Let’s talk about work-up Your CBC is the first clue but it’s not the whole answer. You still need more. 🔬Peripheral smear (a drop of blood spread on a glass slide and examined under a microscope): – In AML, you’ll see circulating blasts (large, immature cells with big
7/ “If the peripheral flow cytometry is diagnostic for AML, do I still need a bone marrow biopsy? … 🤔” Short answer: Yes. Here’s why 👇 Flow cytometry (peripheral blood) → looks at the immunophenotype of the cells (basically, what proteins are on their surface and what the
8/ Logistics of the Bone Marrow Biopsy in AML 🦴 So your patient needs a bone marrow biopsy. But what if they’re unstable? Here’s what matters 👇 – Unstable / ICU patients 🤒→ If they’re crashing and in DIC, the marrow can wait. Stabilize first (fluids, cytoreduction, coags,
9/ Is imaging needed in AML? 🩻 Unlike solid tumors, AML is not staged with CT scans. But imaging does have a role in certain situations: – Neuro symptoms (headache, confusion, focal deficits): Always start with brain imaging (CT/MRI) before doing a lumbar puncture. 👉🏻Why?
10/ Wait, what about APL? 🤔 You’ve probably heard of Acute Promyelocytic Leukemia (APL) which is a unique subtype of AML caused by the t(15;17) translocation that creates the PML-RARA fusion gene. Why it matters: – Patients often present with DIC at diagnosis. – Treatment is
11/ So what do you actually do the moment this patient hits the door with WBC 150k? 🚨 You send the flow cytometry and it shows myeloblasts, yes but stabilization can’t wait. Here’s what matters immediately: –💧IV fluids → Start aggressive hydration (unless contraindicated) to
12/ Management of the Big Three Complications in Acute Leukemia ⚡️ #1: DIC (Disseminated Intravascular Coagulation) DIC is one of the most feared emergencies in AML, especially in APL. Patients can bleed out within hours if not supported. Quick summary of management: – Keep
13/ Management of the Big Three Complications in AML ⚡️ #2: Leukostasis 🧠🫁 Leukostasis = when blasts flood the bloodstream at very high counts (often >100k), turning the blood into sludge. Resulting in poor circulation and clogged microvasculature. How it presents: –
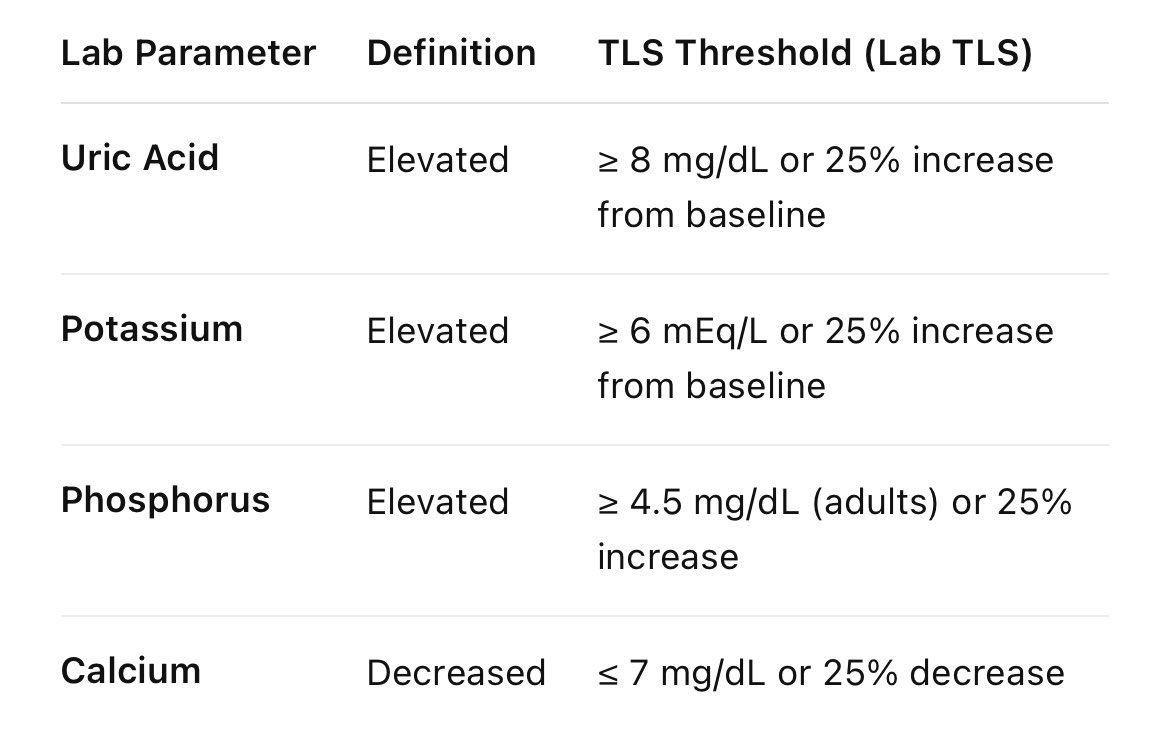
14/ Management of the Big Three Complications in AML ⚡️ #3: Tumor Lysis Syndrome (TLS) TLS = when tumor cells break apart rapidly, dumping their contents into the blood. In AML, this can happen spontaneously (especially with high WBC) or after cytoreduction. Diagnosis
15/ 💭“Do we start antimicrobial prophylaxis right away in AML? …🤔” Short answer: it depends. 👉🏻If the patient is febrile → treat it like neutropenic fever: – Start broad-spectrum antibiotics immediately (e.g. cefepime, piperacillin-tazobactam, or meropenem). – Add
16/ 💭 “So when will hematology actually start treatment for AML? Do we wait for the bone marrow biopsy to come back? 🤔…” The answer: Yes, generally we wait. A bone marrow biopsy is more than just confirming AML, it gives cytogenetics & molecular studies that drive treatment
17/ So what do all these terms mean in acute leukemia management? 🤔 You’ll often hear the heme/onc team talk about induction, consolidation, maintenance, and transplant. Here’s the cheat sheet: Induction: The first, intensive round of therapy aimed at wiping out visible
18/ What does the induction timeline actually look like for AML patients? ⏳ Once a patient is admitted for induction chemo, they’re usually in the hospital for 25–30 days. Here’s why: – Days 1–7 (chemo): Induction (e.g. 7+3) is given. This wipes out the bone marrow. – Days
19/ What should you keep in mind during the long induction stay for AML patients? 🏥 👉 Even after chemo is given, the month-long hospital course has its own challenges. Here are the big ones: ⚡ Tumor Lysis Prophylaxis – Fluids + allo/rasburicase can usually be stopped once
20/ What does discharge prep look like after AML induction? 🏥➡️🏠 Once counts recover (ANC >500 and platelets >20–30k and rising) and the post-induction marrow confirms remission, patients can finally be discharged. Here’s what to keep in mind: – Follow-up: Close outpatient
A final note on AML… ❤️🩹 It’s easy to get caught up in labs, transfusions, chemo regimens, and complications. But don’t forget what AML really means for the patient. Imagine this: your life changes literally overnight. One day you’re at home, the next you’re in the hospital for
And that’s a wrap, folks! That’s it for today. If you’ve been following along, I’m hoping to grow this series into a go-to resource for hospital-based docs navigating hematology oncology cases. Open to suggestions or feedback. If you like this format, like, repost, and share
And if you missed my last episode Tuesday on The Principles of Cancer staging, link below 👇🏻
@hsafaMD Recently lost a pt with APL who presented with spontaneous ic bleed, developed DAH soon after. Couldn’t save her. Sometimes being an icu physician completely feels like a curse. Waiting for your post on APL to know the intricacies Doc, if any.